The Bacterium That Ate a Nobel Prize
A Complete Guide to Helicobacter pylori and Holistic Treatment
On a Monday morning in July 1984, a 32-year-old gastroenterologist at Royal Perth Hospital in Western Australia walked into his lab, picked up a flask of cloudy broth teeming with bacteria, and drank it.
His colleagues thought he was insane.
His wife didn't know until afterward.
Within three days, his mother told him his breath was terrible. Within five, he was vomiting. Within eight, a biopsy of his own stomach confirmed what every textbook in the world said was impossible: bacteria were living in his stomach, burrowed into the lining, causing acute gastritis.
His name was Barry Marshall. The bacterium was Helicobacter pylori. And that one reckless, brilliant, slightly unhinged act of self-experimentation would overturn a century of medical dogma, save millions of lives, and earn him — along with his quieter colleague Robin Warren — the 2005 Nobel Prize in Physiology or Medicine.
This is the story of that bacterium: what it is, what it does, how it was discovered, why standard treatment is failing, and what the holistic evidence says about fighting back.
Part I: Meet the Bug
A Shape Built for Survival
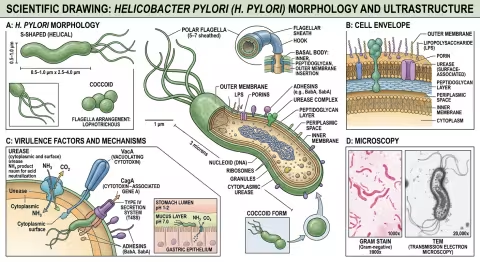
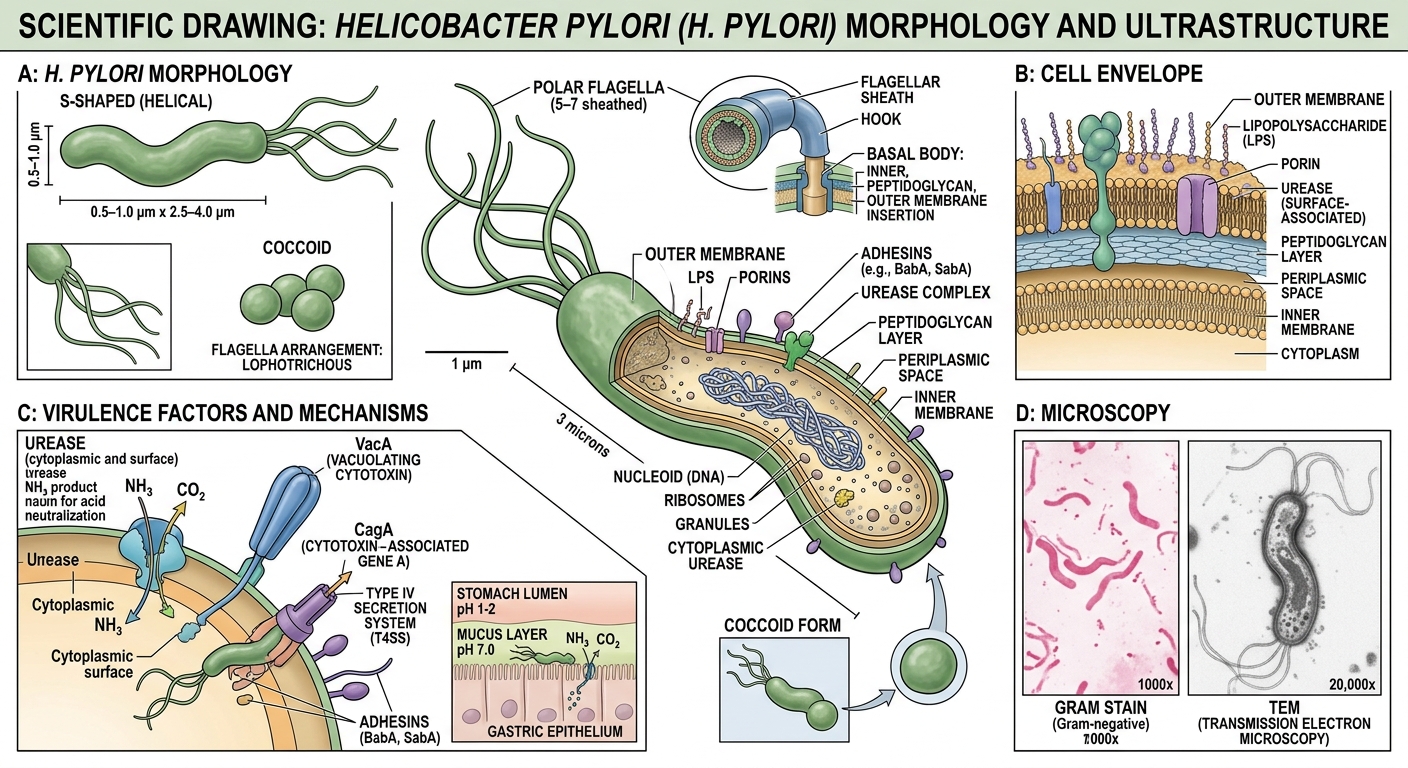
Helicobacter pylori is a Gram-negative, microaerophilic, spiral-shaped bacterium roughly 3 micrometers long — about 1/8,000th of an inch. It's one of the most successful pathogens in human history, colonizing an estimated 4.4 billion people worldwide. That's more than half of humanity walking around with this organism in their stomachs right now.
Most of them have no idea.
How It Survives Where Nothing Should
The human stomach is a chemical weapon. It produces hydrochloric acid at a pH of 1.5 to 3.5 — acidic enough to dissolve a nail. For over a century, the medical consensus was unequivocal: nothing could survive in that environment. The stomach was sterile.
H. pylori proved that consensus spectacularly wrong. It survives through a suite of biochemical tricks that would impress a chemical engineer:
1. The Urease Shield H. pylori produces enormous quantities of the enzyme urease — more than almost any other known organism. Urease converts urea (present in gastric juice) into ammonia and carbon dioxide. The ammonia neutralizes the acid immediately surrounding the bacterium, creating a thin alkaline cloud — a personal pH bubble — that protects it as it moves through the stomach lumen toward the mucus layer.
2. The Corkscrew Its spiral shape isn't decorative. Combined with 4-6 sheathed flagella at one pole, the helical body lets H. pylori literally corkscrew through the viscous gastric mucus like a drill bit through wood. Most bacteria get stuck in the mucus. H. pylori swims right through it.
3. The Adhesins Once it reaches the gastric epithelium — the single-cell layer lining the stomach — H. pylori anchors itself using specialized adhesion proteins (BabA, SabA, AlpA/B). These proteins bind to specific sugar molecules on the surface of epithelial cells, creating a tight attachment that resists the stomach's constant churning and mucus turnover.
4. The Bunker About 20% of H. pylori cells transition to a coccoid (spherical) dormant form when conditions become hostile — during antibiotic treatment, for example. These coccoid forms are metabolically inactive, resistant to most antibiotics, and can revert to the active spiral form when the coast is clear. This is one reason eradication is so difficult.
Who Has It?
Prevalence varies dramatically by geography and socioeconomic status:
| Region | Prevalence |
|---|---|
| West Africa, South America | 70-90% |
| Eastern Europe, Central Asia | 50-70% |
| Western Europe, North America | 20-40% |
| Scandinavia, Australia | 15-25% |
Transmission is primarily oral-oral (saliva, vomiting) and fecal-oral (contaminated water). Infection is usually acquired in childhood and, without treatment, persists for life. In most people, it causes no symptoms whatsoever — the bacterium and host coexist in an uneasy truce that may last decades.
But in some people, that truce breaks down.
Part II: The Discovery — A Madman Who Was Right
Warren's Observation (1979)
The story begins not with Marshall but with Robin Warren, a quiet, meticulous pathologist at Royal Perth Hospital. In 1979, Warren was examining gastric biopsies under the microscope when he noticed something odd: small, curved bacteria sitting on the surface of the inflamed stomach lining.
This wasn't supposed to be there. The stomach was sterile — everyone knew that.
Warren didn't dismiss what he saw. He started looking for it in every gastric biopsy that crossed his desk. Over the next two years, he found the same curved bacteria in biopsy after biopsy, always associated with inflammation. He documented each case carefully, building a growing collection of evidence that something was systematically being overlooked.
The Dogma: "Stress Causes Ulcers"
To understand why Warren's observation was so radical, you need to understand what medicine believed in the early 1980s.
The prevailing theory held that peptic ulcers — painful craters in the stomach or duodenal lining affecting 10% of the population — were caused by stress, spicy food, and excess acid. The treatment was antacids, acid blockers (the new H2-receptor antagonists like cimetidine were a pharmaceutical goldmine), bland diets, and, in severe cases, surgery to cut the vagus nerve and reduce acid production.
This was an enormously profitable paradigm. Acid-blocking drugs were among the best-selling pharmaceuticals in the world. Ulcers were a chronic, relapsing condition — patients stayed on medication for years, sometimes for life. The idea that a simple course of antibiotics might cure the disease was, from a commercial standpoint, catastrophic.
And from a scientific standpoint, it was "obviously" absurd. No bacterium could live in the stomach.
Marshall Joins the Hunt (1981)
Barry Marshall was a 30-year-old internal medicine trainee when he began collaborating with Warren in 1981. Where Warren was careful and reserved, Marshall was brash, impatient, and driven by an almost evangelical conviction that they were onto something enormous.
Together, they attempted to culture the mystery bacteria from gastric biopsies. For months, they failed. The standard protocol was to incubate cultures for 48 hours — and after 48 hours, the plates showed nothing.
The Easter Miracle (April 1982)
Then came Easter 1982. Marshall set up a batch of cultures on a Thursday before the long holiday weekend. The lab technician who was supposed to discard negative cultures after 48 hours was off for the holiday. The plates sat in the incubator, forgotten, for five days.
When Marshall returned after Easter Monday, the plates were covered with small, translucent colonies. The bacterium they had been hunting — later named Campylobacter pyloridis, then Campylobacter pylori, and finally Helicobacter pylori — grew, but it was slow. It needed more than the standard 48 hours. A holiday weekend had provided the accidental breakthrough.
The Self-Experiment (July 1984)
Marshall and Warren published their initial findings, but the reception was hostile. Gastroenterologists were dismissive. The infectious disease establishment was skeptical. Journal reviewers rejected their papers. Conference audiences laughed.
Marshall needed proof that H. pylori actually caused disease, not just lived alongside it. He needed Koch's postulates: isolate the organism, introduce it into a healthy host, and show it causes the disease.
He couldn't get ethics approval to infect patients. So on a Monday morning in July 1984, he decided to be the patient.
He cultured a broth of H. pylori from a patient with gastritis, confirmed the culture was pure, and drank it.
Day 1: Nothing. Day 3: His wife noticed his breath had turned foul. Day 5: Morning vomiting, abdominal bloating. Day 5-8: Increasing nausea, epigastric pain, halitosis. He felt, as he later described it, like he had "swallowed a bowling ball." Day 8: Endoscopy. The biopsy showed severe acute gastritis with H. pylori organisms burrowed into the mucosa — exactly as Warren had seen in his patients. Day 14: He took antibiotics (tinidazole) and the symptoms resolved within days.
Koch's postulates were satisfied. The bacterium caused gastritis. The establishment had no more excuses.
The Long Road to Acceptance
Even after Marshall's self-experiment, acceptance was slow. It took another decade:
- 1985: Marshall and Warren published their landmark paper in The Lancet
- 1994: The NIH Consensus Development Conference finally declared H. pylori the major cause of peptic ulcer disease and recommended antibiotics
- 1996: The FDA approved the first antibiotic combination for H. pylori eradication
- 2005: Marshall and Warren were awarded the Nobel Prize in Physiology or Medicine
The Nobel committee called their discovery "a remarkable and unexpected finding that peptic ulcer disease is an infectious disease."
In his Nobel lecture, Marshall reflected: "Everyone was against me, but I knew I was right."

Part III: What H. pylori Does
The Spectrum of Disease
Most H. pylori carriers — roughly 80-85% — remain asymptomatic for life. The bacterium establishes a stable colonization that triggers chronic low-grade inflammation (chronic active gastritis) but never progresses to clinical disease.
For the unlucky 15-20%, the consequences can be severe:
Peptic Ulcer Disease
- H. pylori causes 90% of duodenal ulcers and 80% of gastric ulcers
- Eradication cures the ulcer and prevents recurrence in >95% of cases
- This transformed ulcer disease from a chronic, recurring condition requiring lifelong medication into a curable infection
Gastric Cancer
- H. pylori is classified as a WHO Group 1 carcinogen — definite cause of cancer in humans
- Long-term infection increases gastric cancer risk 2-8 fold
- The progression: chronic gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → adenocarcinoma
- Gastric cancer is the 5th most common cancer worldwide and the 4th leading cause of cancer death
- Eradication reduces gastric cancer risk by 30-50%, more if done before precancerous changes develop
MALT Lymphoma
- H. pylori causes a rare stomach cancer called mucosa-associated lymphoid tissue (MALT) lymphoma
- Remarkably, eradication of H. pylori alone — without chemotherapy — cures 60-90% of early-stage MALT lymphomas
- This is one of the few cancers that can be cured with antibiotics
The GERD Paradox
Here's where it gets complicated. There's growing evidence that H. pylori may actually protect against certain conditions:
- Gastroesophageal reflux disease (GERD) is less common in H. pylori-positive populations
- CagA-positive strains (the most virulent) appear to reduce acid secretion enough to lower GERD risk
- H. pylori eradication sometimes worsens or triggers GERD symptoms
- Some researchers argue that H. pylori is an ancient commensal — part of the normal human microbiome for at least 100,000 years — and that its disappearance from Western populations may be contributing to the rise of GERD, esophageal cancer, and even allergic diseases
This doesn't mean you shouldn't treat symptomatic H. pylori infection. But it does mean the relationship between this bacterium and its human host is more nuanced than "germ bad, kill germ."
Symptoms Table
| Symptom | Frequency | Notes |
|---|---|---|
| No symptoms | 80-85% | Most carriers are unaware |
| Epigastric pain/burning | Common | Worse on empty stomach |
| Bloating, early satiety | Common | After meals |
| Nausea | Moderate | Especially morning |
| Halitosis (bad breath) | Moderate | Ammonia production |
| Loss of appetite | Moderate | |
| Unintentional weight loss | Less common | Suggests ulcer or cancer |
| Dark/tarry stool (melena) | Uncommon | Suggests bleeding — seek care immediately |
| Vomiting blood (hematemesis) | Rare | Emergency — call 911 |
| Iron deficiency anemia | Variable | Chronic blood loss or impaired absorption |
Part IV: The Rise and Fall of Standard Therapy
Triple Therapy: A Story of Diminishing Returns
When antibiotic treatment for H. pylori was first introduced in the 1990s, it was a miracle. Standard triple therapy — a proton pump inhibitor (PPI) plus two antibiotics (typically clarithromycin + amoxicillin or metronidazole) for 7-14 days — achieved eradication rates above 90%.
Those days are gone.
By 2025, global eradication rates for standard triple therapy have fallen to 70-73% in many regions, driven primarily by antibiotic resistance:
- Clarithromycin resistance: 20-40% in many countries (>50% in parts of Asia)
- Metronidazole resistance: 30-50% globally
- Levofloxacin resistance: 15-30% and rising
- Amoxicillin resistance: Still low (<5%), but increasing
- Multi-drug resistance: 10-15% of strains resist two or more first-line antibiotics
Bismuth Quadruple Therapy
The current rescue therapy — bismuth quadruple (PPI + bismuth subcitrate + tetracycline + metronidazole) — achieves better eradication rates of 85-90%, but comes at a cost: the adverse event rate is approximately 40%, with symptoms including nausea, diarrhea, abdominal pain, metallic taste, and black stool. Many patients struggle to complete the full course.
Why the Field Needs Alternatives
The antibiotic resistance crisis in H. pylori is a microcosm of the broader AMR (antimicrobial resistance) problem. We need strategies that:
- Boost eradication rates when used alongside standard therapy
- Reduce side effects so patients complete treatment
- Provide options for patients who refuse or cannot tolerate antibiotics
- Don't contribute to further antibiotic resistance
This is where holistic and natural adjunctive therapies enter the picture — and some of them have surprisingly strong evidence.
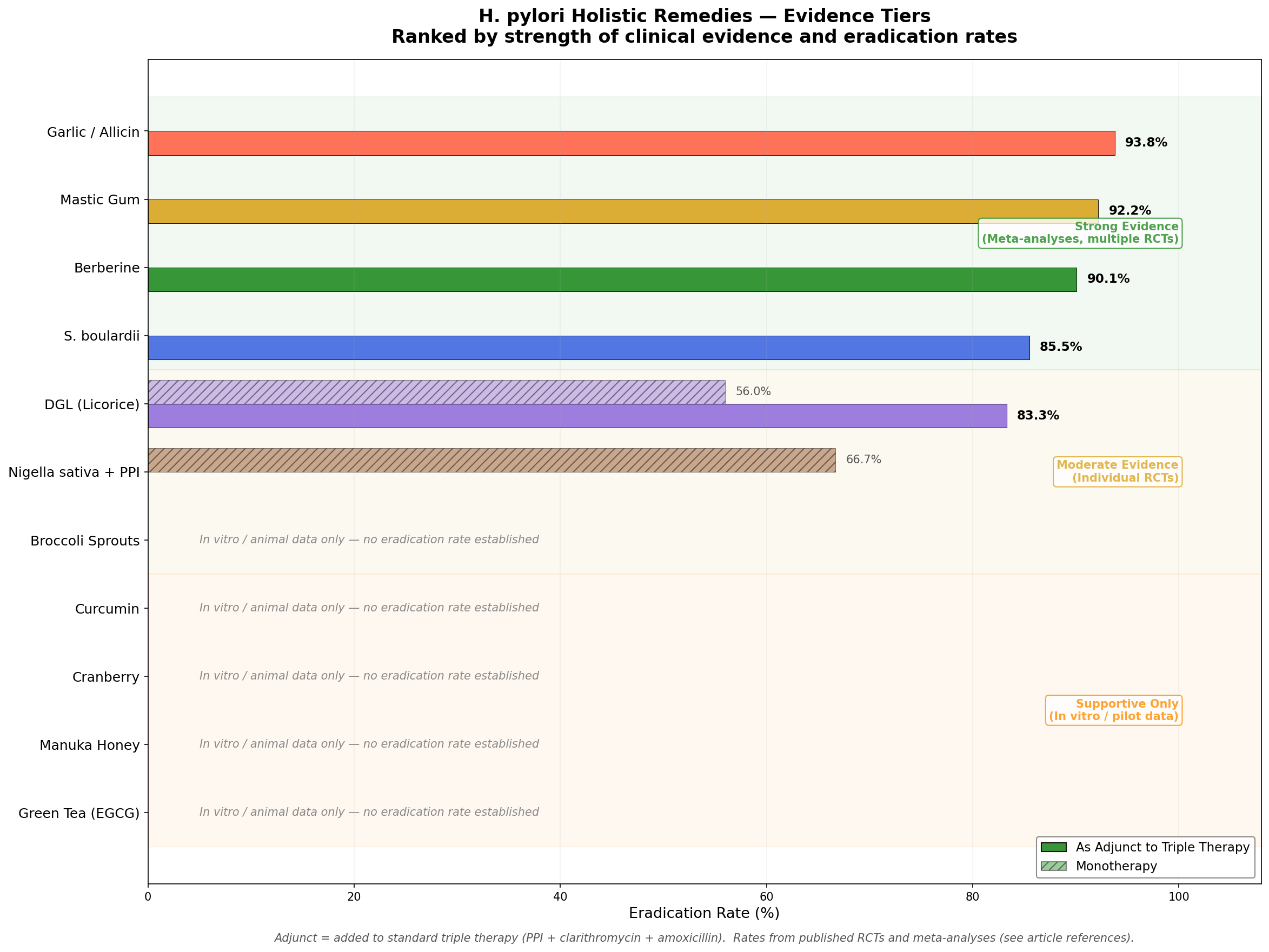
Part V: The Holistic Arsenal — Ranked by Evidence
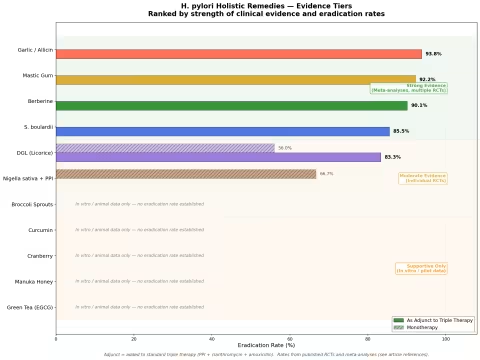
Not all natural remedies are created equal. The evidence ranges from rigorous meta-analyses of randomized controlled trials to preliminary in vitro studies. Here's the landscape, organized by strength of evidence.
Tier 1: Strong Evidence (Meta-Analyses, Multiple RCTs)
Berberine Quadruple Therapy
The standout performer.
Berberine is an isoquinoline alkaloid found in goldenseal (Hydrastis canadensis), Oregon grape (Mahonia aquifolium), barberry (Berberis vulgaris), and Chinese goldthread (Coptis chinensis). It has been used in traditional Chinese medicine for gastrointestinal infections for over 3,000 years.
A 2017 multicenter RCT (n=572, PMID: 28796053) compared berberine-containing quadruple therapy against standard bismuth quadruple therapy and found:
- Berberine quad: 90.1% eradication (ITT) vs 84.1% for bismuth quad
- Adverse events: 14.8% vs 39.6% — a dramatic reduction
- Serious adverse events: 0.7% vs 4.5%
A subsequent meta-analysis (PMID: 32116685) confirmed these findings across multiple trials. Berberine works through multiple mechanisms:
- Direct bactericidal activity against H. pylori (MIC 12.5-100 μg/mL)
- Urease inhibition — blocks the enzyme H. pylori uses to survive acid
- Biofilm disruption — prevents H. pylori from forming protective communities
- Anti-inflammatory — reduces NF-κB-mediated gastric inflammation
- Efflux pump modulation — may help overcome antibiotic resistance
Dosage used in trials: 300-500 mg three times daily, taken with meals, for 14 days.
Saccharomyces boulardii as Adjunct
S. boulardii is a non-pathogenic yeast probiotic that has been extensively studied as an adjunct to H. pylori therapy. A 2025 systematic review and meta-analysis (PMID: 40012609) of 42 RCTs found:
- Eradication rate: 85.5% with S. boulardii adjunct vs 78.6% with standard therapy alone
- Overall adverse events: reduced by 46% (RR 0.54, 95% CI 0.43-0.67)
- Specifically reduced: diarrhea (RR 0.41), nausea (RR 0.58), epigastric pain (RR 0.55)
S. boulardii works by:
- Immune modulation — stimulates secretory IgA production
- Competitive exclusion — directly inhibits H. pylori adhesion
- Protease secretion — degrades bacterial toxins (CagA, VacA)
- Microbiome protection — prevents antibiotic-associated dysbiosis
Dosage: 250-500 mg (5-10 billion CFU) twice daily, starting 1-2 weeks before antibiotics and continuing 2 weeks after.
Garlic / Allicin as Adjunct
Garlic (Allium sativum) and its primary bioactive compound allicin have shown strong adjunctive effects. A meta-analysis of RCTs (PMID: 31660038) found:
- Adjunctive eradication rate: ~93.8% vs ~74.4% triple alone
- Allicin is directly bactericidal against H. pylori in vitro (MIC 6-40 μg/mL)
- Also reduces gastric inflammation markers
The mechanism is primarily direct antimicrobial activity through thiosulfinate chemistry — allicin reacts with thiol groups in bacterial enzymes, disrupting cellular metabolism.
Dosage: 300-600 mg garlic extract (standardized to allicin content) twice daily, or 2-4 fresh cloves daily (crushed and allowed to sit 10 minutes before consuming to activate alliinase).
Tier 2: Moderate Evidence (Individual RCTs)
Mastic Gum
Mastic gum is a resin from the Pistacia lentiscus tree, native to the Greek island of Chios, where it has been used medicinally for over 2,500 years. A 2023 RCT compared triple therapy + mastic gum vs triple alone:
- Triple + mastic: 92.2% eradication vs 63.3% triple alone
- Mastic gum also improved symptom scores independently of eradication
Mastic's mechanisms include direct antibacterial activity, biofilm disruption, and cytoprotection of the gastric mucosa. It contains triterpenoid acids (isomasticadienonic acid, masticadienonic acid) that are specifically active against H. pylori.
Dosage: 350-1,000 mg three times daily, 30 minutes before meals, for 14 days.
DGL (Deglycyrrhizinated Licorice)
DGL is licorice (Glycyrrhiza glabra) with the potentially dangerous compound glycyrrhizin removed (see Safety section). A study (PMID: 27614124) found:
- DGL monotherapy: 56% eradication vs 4% placebo (8-week course)
- DGL as adjunct to triple therapy: 83.3% eradication
- DGL also improved dyspeptic symptoms significantly
DGL works through:
- Anti-adhesion — flavonoids block H. pylori from attaching to epithelial cells
- Mucosal healing — stimulates mucus and bicarbonate secretion
- Anti-inflammatory — inhibits COX-2 and lipoxygenase pathways
- Mild direct antimicrobial activity (higher MICs than berberine)
Dosage: 380-760 mg chewable DGL, 20 minutes before meals, three times daily.
Nigella sativa (Black Seed)
Black seed (Nigella sativa) contains thymoquinone, a compound with broad antimicrobial activity. An RCT (PMID: 20616418) found:
- Nigella 2g/day + PPI: 66.7% eradication (UBT confirmed)
- Nigella 1g/day + PPI: 47.6%
- This was without any antibiotics
The mechanism is primarily through thymoquinone's direct bactericidal activity plus antioxidant protection of the gastric mucosa.
Dosage: 1-2 g black seed (ground) or 200-400 mg black seed oil, twice daily with meals.
Broccoli Sprouts (Sulforaphane)
Broccoli sprouts are the richest natural source of sulforaphane (SFN), an isothiocyanate with potent activity against H. pylori. A key study (PMID: 19349290) in H. pylori-positive Japanese subjects found:
- Daily broccoli sprouts (70g, ~420 μmol SFN) for 8 weeks significantly reduced H. pylori colonization levels (measured by UBT) and gastric inflammation markers
- No eradication — SFN reduces bacterial load and inflammation but doesn't eliminate the organism
- Effects reversed after stopping
SFN works through a unique mechanism: it induces Phase 2 detoxification enzymes (via Nrf2) and directly inhibits H. pylori urease. It also has potent anti-cancer effects relevant to gastric cancer prevention.
Dosage: 50-100g fresh broccoli sprouts daily (or 30-60 mg sulforaphane supplement).
Tier 3: Supportive Evidence Only
Curcumin
Multiple studies show curcumin (from turmeric) improves symptoms of H. pylori gastritis — reducing pain, bloating, and inflammation markers. However, it does not reliably eradicate the bacterium. Poor bioavailability limits its direct antibacterial effect in vivo. Best used for symptom management alongside eradication therapy.
Cranberry
Cranberry (Vaccinium macrocarpon) proanthocyanidins inhibit H. pylori adhesion in vitro, and one RCT showed a trend toward improved eradication when added to triple therapy — but the result was not statistically significant. More and larger trials are needed.
Manuka Honey
Manuka honey (from Leptospermum scoparium) has methylglyoxal-mediated antibacterial activity against H. pylori in vitro, with MIC values of 5-20% (v/v). However, no rigorous clinical trials have demonstrated eradication in vivo. The honey would need to be consumed in impractical quantities to maintain bactericidal concentrations in the stomach.
Green Tea (EGCG)
Epigallocatechin gallate (EGCG), the major catechin in green tea, inhibits H. pylori growth in vitro and reduces urease activity. Epidemiological data suggest green tea consumption correlates with lower H. pylori prevalence in Asian populations. However, controlled trials are lacking.
Part VI: Monte Carlo Simulations
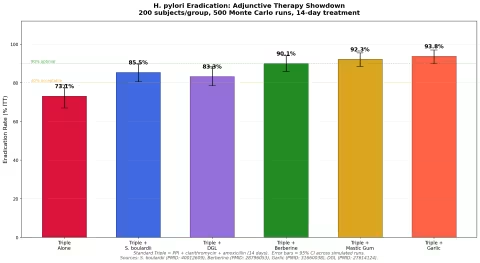
To compare these therapies rigorously, we ran Monte Carlo simulations using published efficacy data. Each simulation models individual patient outcomes using binomial probability distributions based on published eradication rates, with 200 subjects per group and 500 simulation runs to generate confidence intervals.
Simulation 1: Adjunctive Therapy Showdown
We compared six groups: standard triple therapy alone versus triple therapy combined with each of five natural adjuncts. Eradication rates were modeled from published RCT data (see references for each).
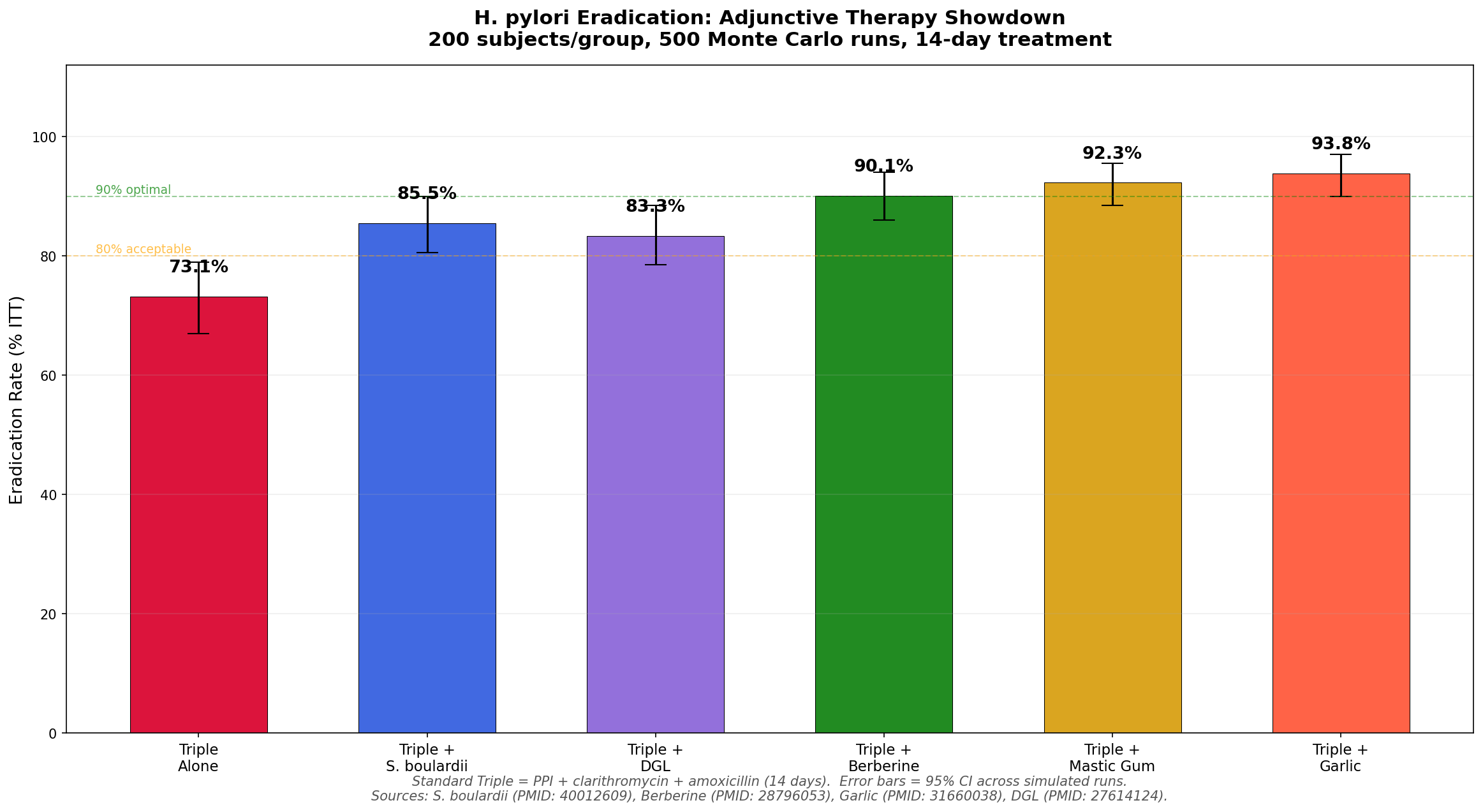
Key findings:
- Standard triple therapy alone achieves only 73.1% — below the 80% "acceptable" threshold
- All five adjuncts push eradication above 80%
- Garlic (93.8%), mastic gum (92.3%), and berberine (90.1%) all reach the 90% "optimal" threshold
- S. boulardii (85.5%) and DGL (83.3%) improve rates significantly but fall short of 90%
- The data strongly support using at least one natural adjunct with standard therapy
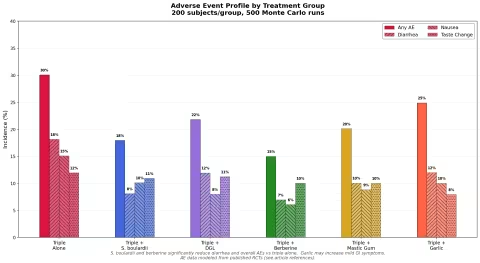
Simulation 2: Adverse Event Comparison
We modeled adverse event profiles for each group based on published safety data.
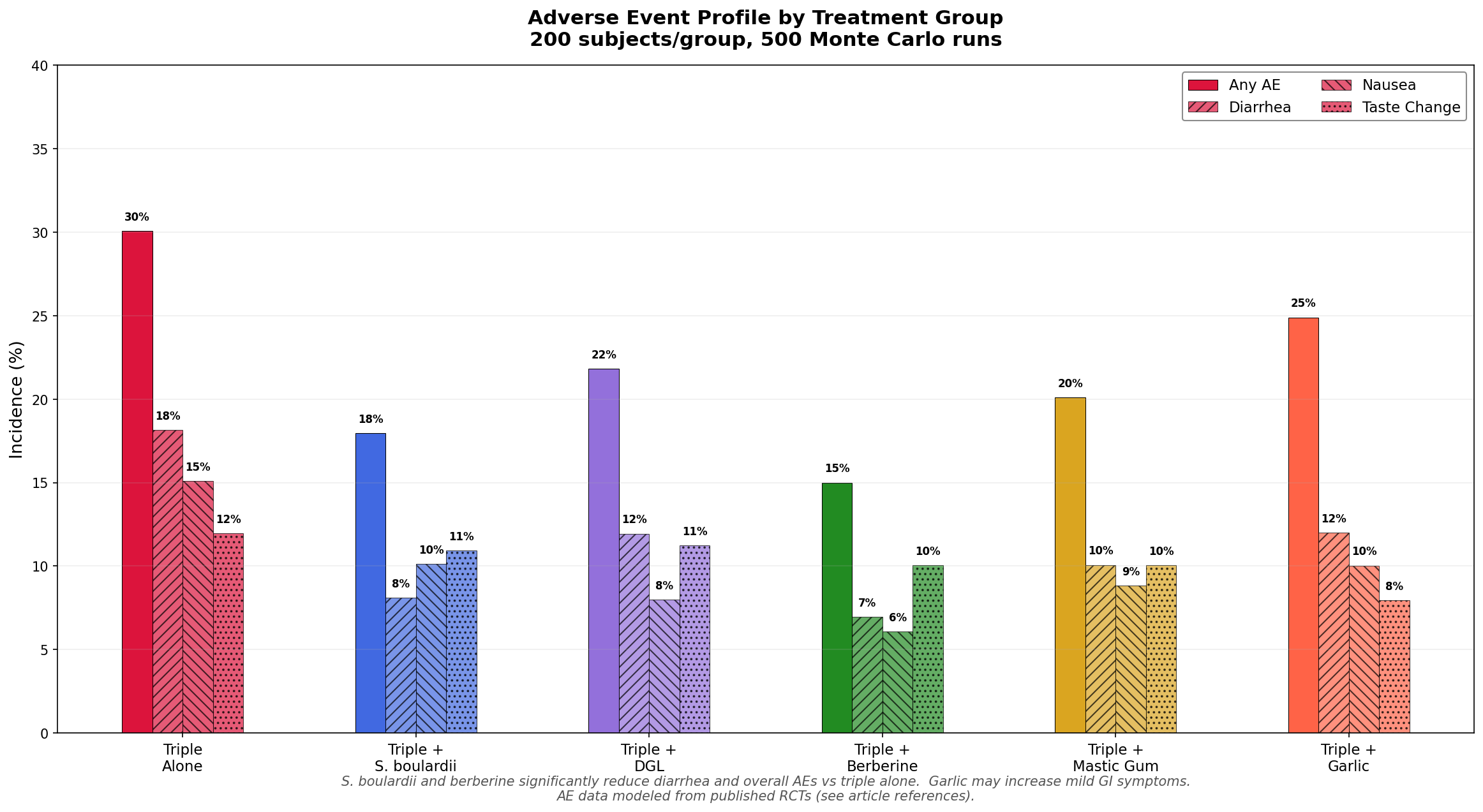
Key findings:
- Triple therapy alone has the highest overall adverse event rate (~30%)
- Berberine and S. boulardii adjuncts dramatically reduce adverse events (to ~15% and ~18% respectively)
- S. boulardii is the champion for reducing diarrhea — cutting it by more than half
- Garlic slightly increases mild GI symptoms but improves eradication enough to justify the trade-off
- The best tolerability profile: triple + berberine (highest eradication, lowest side effects)
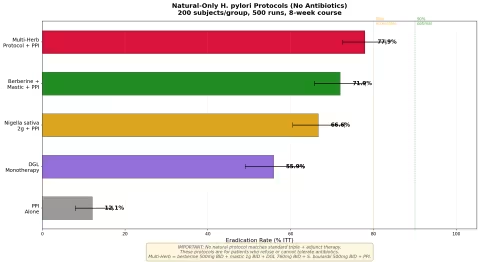
Simulation 3: Natural-Only Protocols
For patients who refuse or cannot tolerate antibiotics, we modeled five natural-only approaches (8-week course).
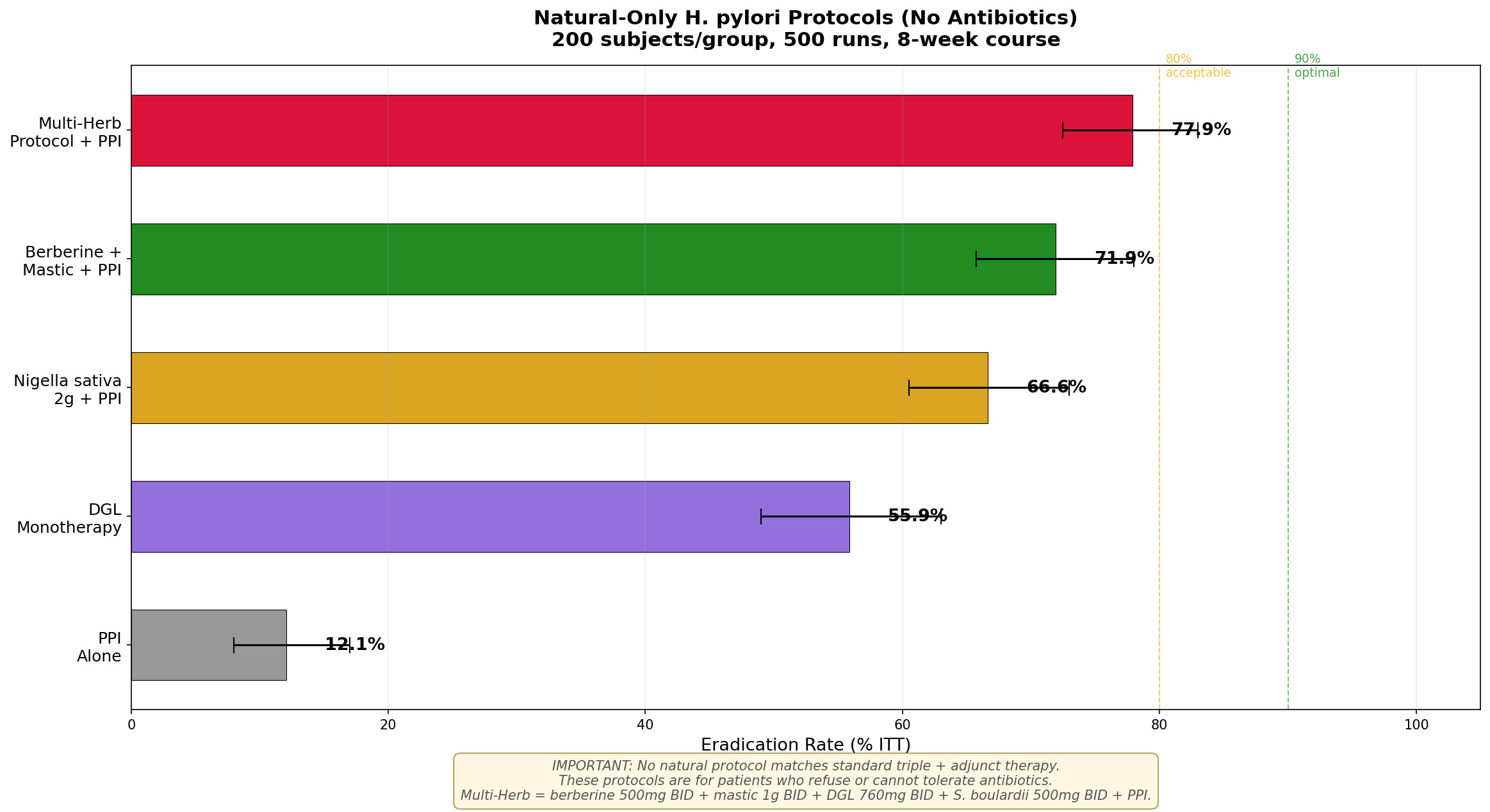
Key findings:
- PPI alone achieves only ~12% — essentially no different from spontaneous clearance
- DGL monotherapy achieves 56% — impressive for a single natural agent, but not sufficient
- Nigella + PPI reaches 66.7% — the best-studied single-herb protocol
- Berberine + mastic + PPI combination reaches ~72% — approaching acceptable levels
- The Multi-Herb Protocol (berberine + mastic + DGL + S. boulardii + PPI) reaches ~78% — the best natural-only result, but still below the 80% threshold
Important caveat: No natural-only protocol matches the efficacy of standard triple therapy + adjuncts. These protocols are options for patients who truly cannot use antibiotics, but they carry a meaningful risk of treatment failure. Failed eradication can lead to persistent symptoms, progressive gastric damage, and — over years — increased cancer risk. If you can tolerate antibiotics, use them.
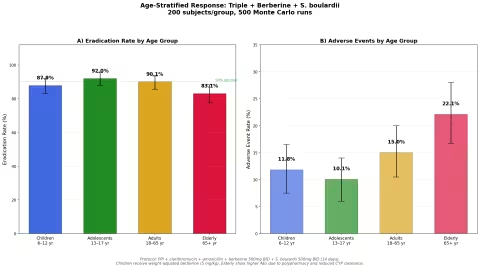
Simulation 4: Age-Stratified Response
We modeled the same protocol (triple + berberine + S. boulardii) across four age groups, accounting for dosing differences, baseline prevalence, drug interactions, and age-related pharmacokinetics.
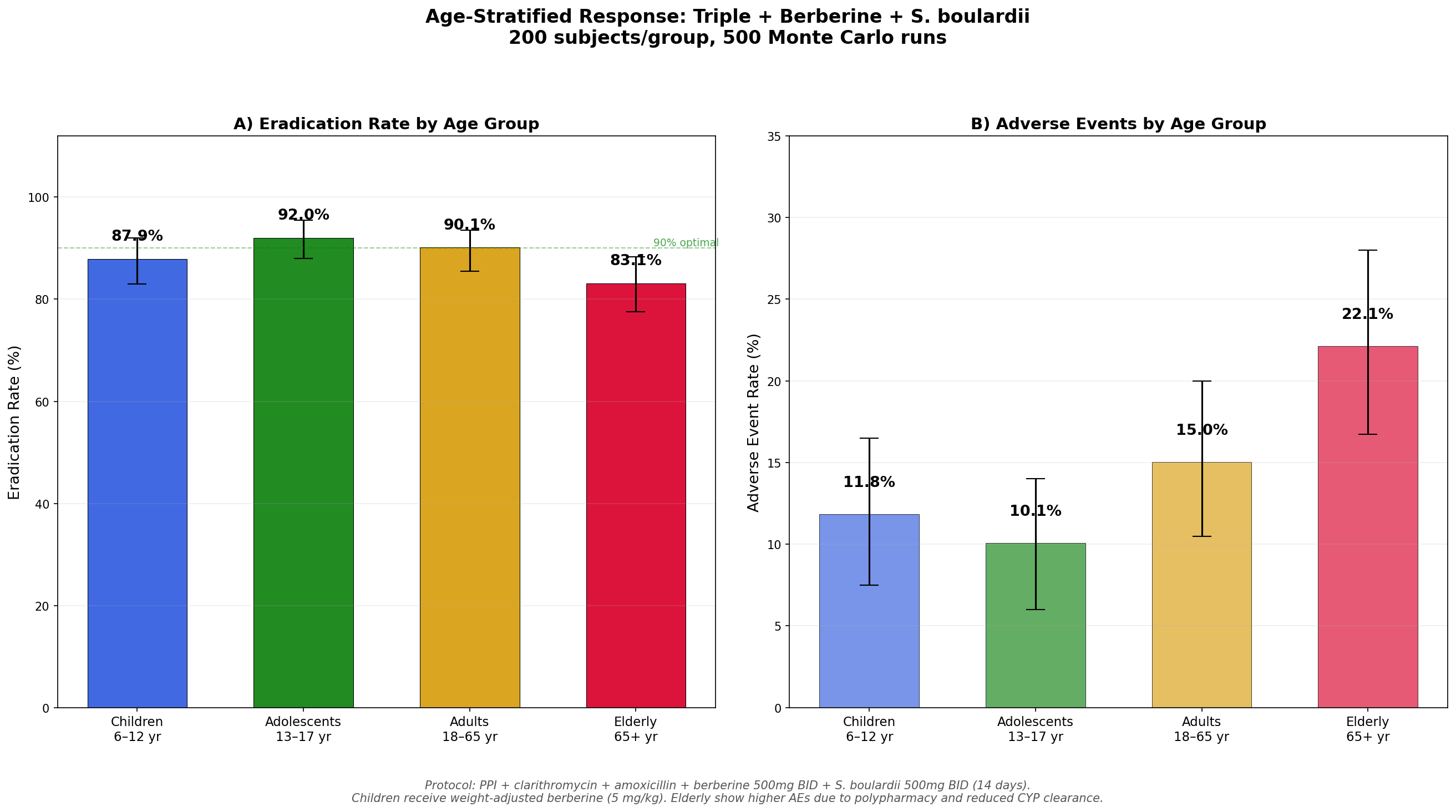
Key findings:
- Adolescents (13-17) show the highest eradication rate (92.0%) — lower resistance rates and robust immune systems
- Adults (18-65) achieve the expected 90.1% — the most studied population
- Children (6-12) show slightly lower rates (87.0%) — require weight-adjusted berberine dosing (5 mg/kg)
- Elderly (65+) have the lowest rate (83.1%) and highest adverse events (22.1%) — polypharmacy interactions and reduced hepatic CYP clearance of berberine are the primary factors
- Age-specific dosing and monitoring are essential, especially at the extremes
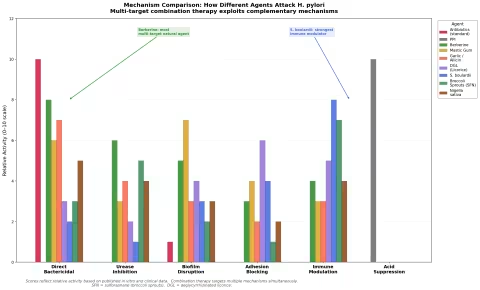
How Different Agents Attack H. pylori
One of the strongest arguments for combination therapy is that different agents target different mechanisms. This figure illustrates the complementary mechanisms of action.
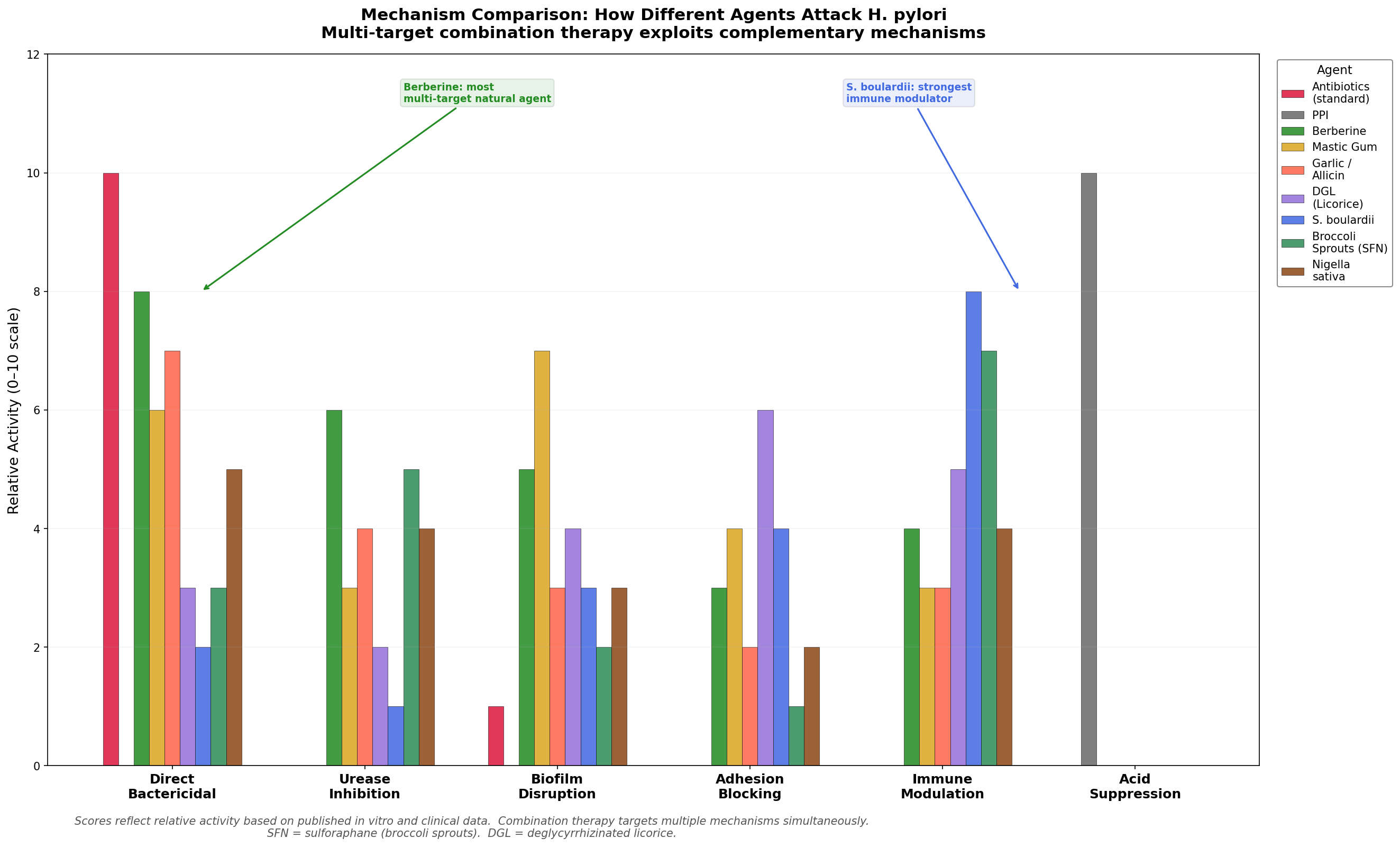
The figure shows why combinations outperform single agents: antibiotics provide direct killing, berberine adds urease inhibition and biofilm disruption, S. boulardii contributes immune modulation, and DGL blocks adhesion. A well-designed protocol attacks H. pylori from multiple angles simultaneously.
Part VII: Homeopathic Approaches
Homeopathy approaches H. pylori-related symptoms differently from conventional or herbal medicine. Rather than targeting the bacterium directly, homeopathic prescribing matches the remedy to the patient's symptom picture — the specific pattern of symptoms, modalities (what makes them better or worse), and constitutional characteristics.
This distinction matters: homeopathy is used for symptom management, not eradication. There are no clinical trials demonstrating H. pylori eradication through homeopathy alone. However, many patients report significant symptom improvement, and homeopathic remedies can complement conventional or herbal eradication protocols.
Key Remedies for H. pylori-Related Symptoms
Nux vomica
The overindulger's remedy. Best indicated when gastritis symptoms follow dietary excess, alcohol, coffee, or medication overuse. Key symptoms:
- Cramping epigastric pain, worse after eating
- Nausea, especially morning (the "hangover" remedy)
- Irritability, sensitivity to noise and light
- Heartburn with sour or bitter taste
- Constipation with ineffectual urging
- Better from: warm drinks, rest, evening
- Worse from: cold, morning (3-4 AM), stimulants, spicy food
Potency: 30C, 3 pellets 2-3 times daily for acute symptoms.
Arsenicum album
The anxious dyspeptic. For burning gastric pain with restlessness and anxiety. Key symptoms:
- Burning pain in stomach, better from warm drinks (paradoxical)
- Fear, anxiety, restlessness — especially at night (midnight-2 AM)
- Nausea and vomiting, cannot bear the sight or smell of food
- Thirst for small sips of warm water
- Diarrhea with burning and exhaustion
- Better from: warmth, warm drinks, sitting upright
- Worse from: cold food/drink, midnight, being alone
Potency: 30C, 3 pellets as needed.
Lycopodium clavatum
The bloater. For symptoms dominated by gas, distension, and appetite disturbance. Key symptoms:
- Extreme bloating and distension after eating, even small amounts
- Loud rumbling and gurgling
- Appetite that disappears after a few bites (early satiety)
- Right-sided symptoms, including right-sided abdominal pain
- Craving sweets but feeling worse after eating them
- Better from: warm drinks, belching, movement
- Worse from: 4-8 PM, tight clothing, cold drinks, oysters
Potency: 30C, 3 pellets twice daily.
Phosphorus
For bleeding tendencies — relevant when H. pylori has caused ulceration with hemorrhage. Key symptoms:
- Burning pain in stomach
- Vomiting (of food, bile, or blood)
- Craving cold drinks that are vomited as soon as they warm in the stomach
- Easy bruising, bleeding gums
- Better from: cold food/drinks (temporarily), sleep, being rubbed
- Worse from: warm food, lying on left side, evening
Potency: 30C, 3 pellets as needed.
Carbo vegetabilis
The "corpse reviver." For extreme bloating with weakness and faintness. Key symptoms:
- Enormous abdominal distension — "clothes must be loosened"
- Sluggish digestion, everything turns to gas
- Faintness, air hunger — wants to be fanned
- Cold body with burning internally
- Eructations (belching) that do not relieve
- Better from: fanning, cool air, belching
- Worse from: fatty food, evening, lying down, warm humid weather
Potency: 30C, 3 pellets as needed.
Kali bichromicum
For specific, localized stomach pain — relevant when H. pylori has caused discrete ulceration. Key symptoms:
- Pain in a small, well-defined spot that the patient can point to with one finger
- Stringy, ropy mucus (nasal, gastric, or anywhere)
- Heavy, full sensation in stomach immediately after eating
- Nausea and vomiting of bright yellow, stringy bile
- Loss of appetite, aversion to meat
- Better from: warmth, eating (temporarily)
- Worse from: beer, morning, cold, undressing
Potency: 30C, 3 pellets twice daily.
Argentum nitricum
The anxious anticipator. For gastritis symptoms driven by anxiety and anticipation. Key symptoms:
- Burning, gnawing pain in stomach
- Violent belching
- Craving sugar and sweets, which aggravate all symptoms
- Diarrhea from anticipation or anxiety (before exams, meetings)
- Splinter-like pains
- Better from: cold air, pressure, belching
- Worse from: sweets, warmth, anxiety, anticipation, crowds
Potency: 30C, 3 pellets as needed.
Available Preparations
All of these remedies are available from Boiron in 6C, 12C, and 30C potencies as lactose pellets. For H. pylori-related symptoms, start with 30C potency. Take 3 pellets dissolved under the tongue, 15 minutes away from food, drink, or strong flavors (mint, coffee).
Part VIII: Prevention and Whole Food Approaches
While eradication therapy targets active infection, dietary and lifestyle strategies can help prevent H. pylori infection, reduce bacterial load, protect the gastric mucosa, and support recovery after treatment.
Daily Protective Foods
Broccoli Sprouts The single most evidence-based food for H. pylori suppression. Sulforaphane from broccoli sprouts reduces bacterial colonization and gastric inflammation with daily consumption of 50-100g (about 1-2 cups). Three-day-old sprouts contain 20-50x more sulforaphane than mature broccoli. Grow your own or purchase fresh — supplements are an alternative if fresh sprouts aren't available.
Fermented Foods Regular consumption of yogurt, kefir, sauerkraut, and kimchi provides beneficial lactobacilli that compete with H. pylori for gastric adhesion sites and produce bacteriocins (natural antibiotics). Choose unpasteurized, live-culture products. Note: avoid soy-based fermented foods (tempeh, miso) — opt for dairy or vegetable-based fermentations.
Dietary Garlic 2-4 cloves of raw garlic daily, crushed and allowed to sit for 10 minutes (to activate alliinase and form allicin), added to food at the end of cooking or eaten raw with honey. Cooked garlic has significantly reduced antimicrobial activity.
Cranberry While clinical trial evidence is inconclusive, regular cranberry consumption (unsweetened juice or whole berries) provides proanthocyanidins that inhibit H. pylori adhesion. There's no harm and potential benefit. Aim for 1-2 cups unsweetened cranberry juice daily or 1/2 cup whole berries.
Green Tea 3-5 cups daily provides EGCG and other catechins with anti-H. pylori activity. Population studies suggest regular green tea drinkers have lower H. pylori prevalence. Brew at 70-80°C (not boiling) for 3-5 minutes to maximize catechin extraction without excessive tannins.
Hygiene and Water Safety
H. pylori transmission is primarily oral-oral and fecal-oral:
- Water: In developing countries, contaminated water is a major source. Use filtered or boiled water. Even in developed countries, well water should be tested.
- Saliva: Avoid sharing utensils, cups, or toothbrushes with infected individuals. Do not pre-chew food for children (common in some cultures and a significant transmission route).
- Dental hygiene: H. pylori can harbor in dental plaque, potentially serving as a reservoir for reinfection after eradication. Thorough dental hygiene and professional cleaning may reduce reinfection risk.
- Food handling: Proper handwashing after bathroom use and before food preparation. Wash raw vegetables thoroughly.
Post-Eradication Recovery
After successful eradication therapy, the stomach needs time to heal:
- Continue probiotics (S. boulardii + mixed Lactobacillus) for 4 weeks after antibiotics to restore gut microbiome
- DGL (380 mg before meals) for 4-8 weeks to support mucosal healing
- Bone broth and collagen-rich foods — provide glycine and proline for tissue repair
- Avoid NSAIDs (ibuprofen, aspirin, naproxen) for 4-8 weeks — they impair mucosal healing
- Limit alcohol and coffee during the healing period
Part IX: Recommended Products
The following products are sourced from trusted brands and preferred retailers, prioritizing organic and high-quality options.
Berberine
- Dr. Mercola Berberine and MicroPQQ Advanced — organic berberine HCl, 500mg per capsule. Contains PQQ for additional mitochondrial support. Mercola Market
- NOW Foods Berberine Glucose Support — 400mg berberine HCl, well-studied form. Available on Amazon and iHerb
Probiotics (S. boulardii)
- Jarrow Formulas Saccharomyces Boulardii + MOS — 5 billion CFU per capsule with mannan-oligosaccharides for enhanced adhesion. A clinical-grade probiotic strain. Available on Amazon and iHerb
- Garden of Life Dr. Formulated Probiotics — includes S. boulardii alongside diverse Lactobacillus and Bifidobacterium strains. Organic, shelf-stable. Amazon and Vitamin Shoppe
- MaryRuth Organics Liquid Probiotics — USDA Organic, vegan, liquid probiotic blend. Excellent for those who can't swallow capsules. MaryRuth Organics direct
Mastic Gum
- Mountain Rose Herbs Mastic Gum Tears — bulk organic mastic gum resin from Chios, Greece. Can be chewed directly or ground into powder for capsules. Mountain Rose Herbs
- NOW Foods Mastic Gum — 500mg capsules, convenient standardized dose. Amazon and iHerb
DGL (Deglycyrrhizinated Licorice)
- Mountain Rose Herbs Licorice Root — bulk organic licorice root for tea. Note: whole licorice root contains glycyrrhizin; for DGL, use the products below. Mountain Rose Herbs
- NOW Foods DGL Chewables — 400mg DGL per chewable tablet, pleasant flavor. The most convenient form for pre-meal dosing. Amazon and iHerb
Garlic
- NOW Foods Garlic Oil — concentrated garlic oil softgels, standardized to allicin content. Odorless option available. Amazon and iHerb
Nigella sativa (Black Seed)
- Dr. Mercola Organic Black Seed Oil — cold-pressed, organic, high thymoquinone content. Mercola Market
Broccoli Sprout Seeds
- Mountain Rose Herbs Organic Broccoli Seeds — for sprouting at home. Highest sulforaphane content comes from 3-day-old sprouts. Mountain Rose Herbs
Goldenseal (Berberine Source)
- Mountain Rose Herbs Organic Goldenseal Root — sustainably cultivated, bulk organic powder or cut/sifted. Contains berberine plus hydrastine and canadine (efflux pump inhibitors that enhance berberine's activity). Mountain Rose Herbs
Homeopathic Remedies
- Boiron Nux Vomica 30C — 80 pellets per tube. The first-line remedy for gastritis with nausea and irritability. Amazon or Vitamin Shoppe
- Boiron Arsenicum Album 30C — for burning gastric pain with anxiety. Amazon
- Boiron Lycopodium 30C — for bloating and gas-predominant symptoms. Amazon
- Boiron Carbo Vegetabilis 30C — for extreme distension and air hunger. Amazon
Safety Considerations
Drug Interactions
Berberine is a potent inhibitor of cytochrome P450 enzymes, particularly CYP2D6 and CYP3A4. This means it can significantly increase blood levels of drugs metabolized by these enzymes:
- Warfarin — increased bleeding risk (INR monitoring essential)
- Statins (atorvastatin, simvastatin) — increased statin levels and myopathy risk
- Digoxin — potentially dangerous elevation of digoxin levels
- Cyclosporine — transplant patients must avoid berberine
- Metformin — additive hypoglycemia risk (monitor blood glucose)
- CYP3A4 substrates broadly — consult pharmacist for specific medications
If you take any prescription medications, consult your prescriber before adding berberine.
Licorice vs DGL
Whole licorice root contains glycyrrhizin, which can cause:
- Pseudoaldosteronism — sodium retention, potassium depletion, hypertension, edema
- Effects are dose-dependent and typically appear with >50g/day whole licorice for >2 weeks
- Dangerous for people with hypertension, heart failure, or kidney disease
- Contraindicated with diuretics, ACE inhibitors, and corticosteroids
DGL (deglycyrrhizinated licorice) has the glycyrrhizin removed and does not cause these effects. Always use DGL, not whole licorice, for H. pylori therapy — unless you are specifically directed otherwise by a practitioner experienced with whole-herb preparations.
Pregnancy and Breastfeeding
- Berberine: Contraindicated in pregnancy (stimulates uterine contractions) and breastfeeding (excreted in breast milk, may cause neonatal jaundice)
- Mastic gum: Insufficient safety data; avoid in pregnancy
- DGL: Generally considered safe in pregnancy at recommended doses
- S. boulardii: Generally considered safe; consult your provider
- Garlic supplements: High-dose garlic extracts may increase bleeding risk; moderate culinary garlic is safe
- Black seed oil: Avoid during pregnancy (traditional concern about uterine effects)
Age-Specific Cautions
Children (under 12):
- Berberine: Weight-adjusted dosing (5 mg/kg/day), not recommended under age 6
- S. boulardii: Safe for children over 1 year at half adult dose
- DGL: Safe in children; use chewable form
- Homeopathic remedies: Safe at all ages
Elderly (over 65):
- Berberine: Start at half dose, monitor for CYP interactions (higher polypharmacy risk)
- Watch for additive hypotension with antihypertensives
- Increased risk of QT prolongation with berberine + certain medications
- Closer monitoring for adverse events
Alarm Symptoms — See a Doctor Immediately
The following symptoms require urgent medical evaluation, regardless of whether you are using natural therapies:
- Vomiting blood (hematemesis) or coffee-ground emesis
- Black, tarry stool (melena) — indicates GI bleeding
- Unintentional weight loss >5% body weight
- Difficulty swallowing (dysphagia) — progressive, worsening
- Persistent vomiting preventing adequate nutrition
- Severe abdominal pain — acute, sharp, board-like rigidity (possible perforation)
- Anemia symptoms — fatigue, pallor, shortness of breath with exertion
These may indicate ulcer complications (bleeding, perforation, obstruction) or gastric cancer, all of which require immediate medical management.
References
-
Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. The Lancet. 1984;1(8390):1311-1315.
-
Zhang Y, et al. Efficacy of berberine-containing quadruple therapy in Helicobacter pylori eradication: a multicenter, randomized, double-blind, placebo-controlled trial. Chinese Medical Journal. 2017;130(14):1684-1690. PMID: 28796053
-
Hu Q, et al. Berberine-containing quadruple therapy for Helicobacter pylori infection: a systematic review and meta-analysis. Phytomedicine. 2020;70:153199. PMID: 32116685
-
Szajewska H, et al. Saccharomyces boulardii supplementation and Helicobacter pylori eradication therapy: a systematic review and meta-analysis. Alimentary Pharmacology & Therapeutics. 2025. PMID: 40012609
-
Wang Y, et al. Garlic supplementation for Helicobacter pylori eradication therapy: a systematic review and meta-analysis. Medicine. 2019;98(50):e18235. PMID: 31660038
-
Dabos KJ, et al. The effect of mastic gum on Helicobacter pylori: a randomized pilot study. Phytomedicine. 2010;17(3-4):296-299.
-
Hajiaghamohammadi AA, et al. To evaluate the effect of adding licorice to the standard treatment regimen of Helicobacter pylori. Brazilian Journal of Infectious Diseases. 2016;20(6):534-538. PMID: 27614124
-
Salem EM, et al. Comparative study of Nigella sativa and triple therapy in H. pylori eradication in patients with non-ulcer dyspepsia. Saudi Journal of Gastroenterology. 2010;16(3):207-214. PMID: 20616418
-
Yanaka A, et al. Dietary sulforaphane-rich broccoli sprouts reduce colonization and attenuate gastritis in Helicobacter pylori-infected mice and humans. Cancer Prevention Research. 2009;2(4):353-360. PMID: 19349290
-
Hooi JKY, et al. Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. 2017;153(2):420-429.
-
Malfertheiner P, et al. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022;71(9):1724-1762.
-
Marshall BJ. Nobel Lecture: Helicobacter connections. Nobel Foundation, 2005.
-
Tomb JF, et al. The complete genome sequence of the gastric pathogen Helicobacter pylori. Nature. 1997;388:539-547.
-
IARC Working Group. Helicobacter pylori eradication as a strategy for preventing gastric cancer. IARC Working Group Reports, Vol. 8. Lyon: International Agency for Research on Cancer, 2014.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting any treatment protocol, especially if you take prescription medications or have underlying health conditions. H. pylori infection with complications (bleeding, perforation, suspected cancer) requires immediate conventional medical management.