Nature's Metformin
A Complete History, Science, and Healing Guide to Berberine
In 2008, a team of Chinese researchers did something outrageous. They took 116 newly diagnosed type 2 diabetics, split them into two groups, gave one group berberine — an alkaloid from a plant root — and the other group metformin — the world's most prescribed diabetes drug — and waited three months.
The results were identical.
Berberine reduced HbA1c by 0.9%. Metformin reduced it by 0.97%. Berberine dropped fasting blood glucose by 25.9%. Metformin dropped it by 27.4%. The differences were not statistically significant. A plant compound that costs pennies to produce, available without prescription, extracted from roots that Chinese doctors had been prescribing for 3,000 years, had just matched the gold-standard pharmaceutical for the world's fastest-growing metabolic disease.
Then the researchers looked at the lipid data. Berberine dropped triglycerides by 35.9%. Metformin dropped them by 6.3%. Berberine crushed LDL by 21%. Metformin managed 7.3%. For lipids, berberine didn't just match metformin — it destroyed it.
That study, led by Jun Yin at Shanghai Jiao Tong University, set off a cascade of research that has produced over 5,000 published papers in the last 15 years. The mechanism turned out to be the same one metformin uses: AMPK activation — flipping the master metabolic switch that tells every cell in your body to burn fuel more efficiently, absorb glucose, oxidize fat, and reduce inflammation. Berberine and metformin are doing the same thing through different chemistry.
But berberine does things metformin can't. It lowers cholesterol through a completely separate mechanism (upregulating LDL receptors — the same pathway statins use). It remodels the gut microbiome, selectively suppressing pathogenic bacteria while promoting beneficial species. It reverses fatty liver. It kills antibiotic-resistant bacteria. It inhibits cancer cell proliferation through at least five independent pathways. And it's been doing all of this, in clinical use, since before Hippocrates was born.
This is the story of berberine — the bright yellow alkaloid hiding inside goldenseal, barberry, Oregon grape, and a Chinese root called huang lian — and the remarkable convergence of 5,000 years of traditional medicine with 21st-century molecular biology.
Part I: What Berberine Is (and Isn't)
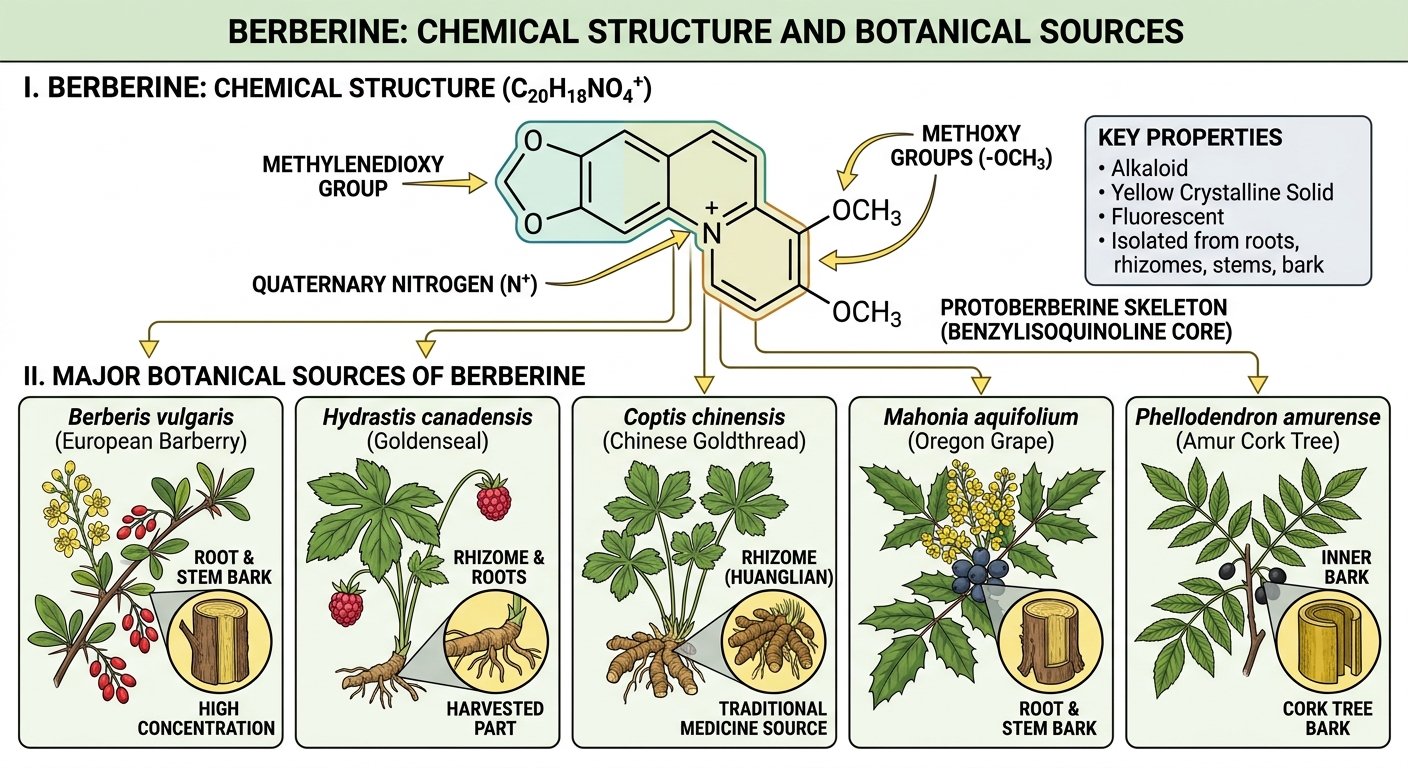
The Molecule
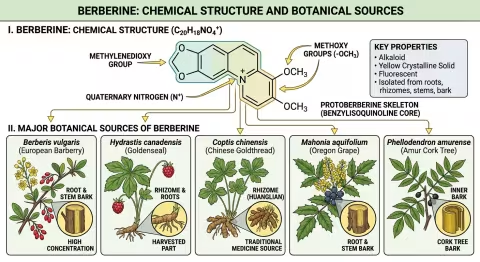
Berberine is an isoquinoline alkaloid — a nitrogen-containing organic compound with a distinctive bright yellow color. Its IUPAC name is 5,6-dihydro-9,10-dimethoxy-1,3-dioxolo[4,5-g]isoquinolino[3,2-a]isoquinolin-7-ium, but nobody calls it that. They call it berberine.
| Property | Detail |
|---|---|
| Chemical formula | C₂₀H₁₈NO₄⁺ |
| Molecular weight | 336.36 g/mol |
| Color | Bright yellow (fluorescent under UV) |
| Taste | Intensely bitter |
| Solubility | Poorly water-soluble; better in ethanol and acidic solutions |
| Bioavailability | Low (~5%) — a significant clinical consideration |
| Half-life | ~2–4 hours (requiring multiple daily doses) |
That bright yellow color is berberine's calling card. If you've ever seen goldenseal root, Oregon grape root, or barberry bark, you've noticed the vivid yellow stain — that's berberine. It was used as a textile dye across Asia for centuries before anyone catalogued its medicinal properties.
The Plants That Make It
Berberine isn't a plant — it's a compound produced by at least 12 plant families as a chemical defense against microbial pathogens and herbivores. The major medicinal sources:
| Plant | Common Name | Family | Berberine Content | Traditional System |
|---|---|---|---|---|
| Coptis chinensis | Huang lian (Chinese goldthread) | Ranunculaceae | 5–8% (root) | TCM — primary source |
| Berberis vulgaris | Common barberry | Berberidaceae | 2–5% (root bark) | Unani, European herbal |
| Berberis aristata | Indian barberry (daruharidra) | Berberidaceae | 3–5% (root/stem bark) | Ayurveda |
| Hydrastis canadensis | Goldenseal | Ranunculaceae | 2.5–4.5% (root) | Native American, Eclectic |
| Mahonia aquifolium | Oregon grape | Berberidaceae | 1–3% (root bark) | Native American |
| Phellodendron amurense | Huang bai (Amur cork tree) | Rutaceae | 1.5–3% (bark) | TCM |
| Tinospora cordifolia | Guduchi | Menispermaceae | 0.5–1% (stem) | Ayurveda |
The fact that such distantly related plant families — buttercups, barberries, rue, moonseed — all independently evolved the ability to produce berberine is a powerful signal. It means berberine confers such a strong survival advantage (antimicrobial defense) that evolution invented it multiple times. When nature converges on the same molecule across unrelated lineages, the molecule is doing something important.
For a deeper exploration of goldenseal — one of the most important berberine sources and a fascinating medicinal plant in its own right — see our complete goldenseal guide.
Berberine vs. Its Plant Sources: An Important Distinction
A critical point that supplement marketing often obscures: berberine is not goldenseal, and goldenseal is not berberine. Each berberine-containing plant produces a unique cocktail of alkaloids and other compounds that modify berberine's effects:
- Goldenseal contains berberine plus hydrastine and canadine — alkaloids with independent antimicrobial and anti-inflammatory activity. The whole-root extract has documented synergistic effects that isolated berberine doesn't replicate.
- Coptis chinensis contains berberine plus coptisine, palmatine, and jatrorrhizine — which together provide broader antimicrobial coverage than berberine alone.
- Barberry contains berberine plus berbamine — a compound with distinct anti-inflammatory and immunomodulatory effects.
For targeted metabolic effects (blood sugar, cholesterol, fatty liver), isolated berberine supplements are well-studied and effective. For antimicrobial and gut applications, whole-plant extracts may offer advantages through alkaloid synergy. Both approaches have valid evidence behind them.
Part II: 5,000 Years of the Golden Alkaloid
Ancient China: Huang Lian (~3000 BCE – 200 CE)
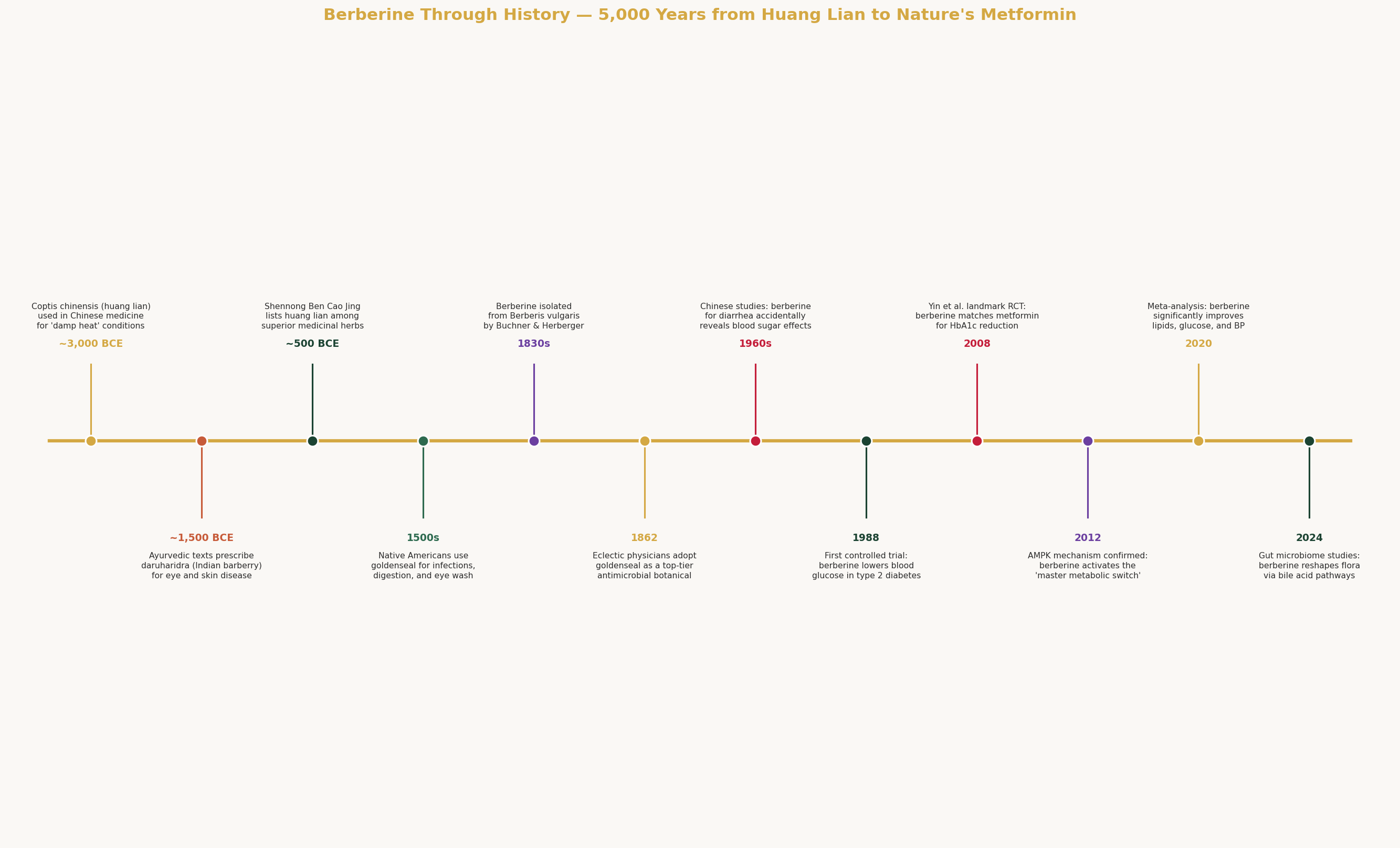
The oldest documented use of berberine-containing plants comes from Traditional Chinese Medicine, where Coptis chinensis (huang lian — "yellow connection") has been prescribed for at least 3,000 years.
The Shennong Ben Cao Jing (Divine Farmer's Materia Medica, compiled ~200 CE from oral traditions dating to ~3000 BCE) classifies huang lian among the superior herbs (shang pin) — the highest tier, reserved for medicines that "nourish life" and can be taken long-term without toxicity. It was prescribed for:
- "Damp heat" conditions — the TCM diagnostic category that maps onto what we'd now call infections, inflammation, and metabolic dysfunction
- Intestinal complaints — dysentery, diarrhea, abdominal pain
- Eye infections — conjunctivitis, trachoma
- Skin conditions — abscesses, boils, infected wounds
- "Fire toxin" — febrile illness, toxic heat patterns
The TCM classification is remarkably prescient. "Damp heat" — the combination of excess moisture and inflammatory heat — describes precisely the pathological state that berberine treats: metabolic syndrome (excess adiposity + systemic inflammation), infectious diarrhea (microbial overgrowth + intestinal inflammation), and skin infections (bacterial/fungal colonization + inflammatory response). The ancient diagnostic framework and the modern molecular mechanisms are describing the same biology in different languages.
Huang lian remained one of the most frequently prescribed single herbs in Chinese medicine for three millennia. It appears in foundational formulas including:
- Huang Lian Jie Du Tang (Coptis Detoxification Decoction) — for "fire toxin" in all three burners (roughly: systemic infection with high fever)
- Ge Gen Huang Qin Huang Lian Tang — for acute dysentery with fever
- Zuo Jin Wan — for acid reflux and stomach fire (berberine's gastroprotective effects predate our understanding of gastric acid by 2,000 years)
Ayurveda: Daruharidra (~1500 BCE)
In Ayurvedic medicine, Berberis aristata — known as daruharidra (literally "wood turmeric," named for its yellow color resembling turmeric) — has been prescribed since at least the era of the Charaka Samhita (~700 BCE, based on earlier oral traditions).
Ayurvedic classification:
- Rasa (taste): Bitter, astringent
- Virya (energy): Hot
- Vipaka (post-digestive): Pungent
- Dosha effect: Reduces Kapha and Pitta (excess moisture and inflammation — the same "damp heat" that TCM identified)
Ayurvedic indications:
- Prameha (urinary disorders including diabetes) — remarkably, Ayurveda classified conditions with sweet urine (glucosuria) as treatable with daruharidra over 2,000 years before berberine's blood-sugar-lowering mechanism was discovered
- Eye diseases (netra roga) — berberine-containing eye washes were prescribed for conjunctivitis and trachoma
- Skin diseases (kushtha) — topical and oral preparations for infected dermatoses
- Digestive disorders — diarrhea, dysentery, intestinal parasites
- Liver diseases (yakrit vikara) — hepatoprotective applications that align with modern NAFLD research
- Wound healing — topical antiseptic
Two medical systems, developed independently on opposite sides of the Himalayas, arrived at virtually identical clinical applications for the same molecule. That's not coincidence — that's convergent empirical observation over thousands of patient-years.
Native American Medicine (Pre-1500s – 1800s)
At least six Native American tribes used berberine-containing plants medicinally:
- Cherokee: Goldenseal (Hydrastis canadensis) root as an eye wash for conjunctivitis, a digestive bitter for stomach complaints, and a wash for skin infections and wounds
- Iroquois: Goldenseal for whooping cough, liver disorders, and fever
- Micmac: Goldenseal infusion for mouth ulcers and sore throat
- Various Pacific Northwest tribes: Oregon grape (Mahonia aquifolium) root bark for digestive complaints, infections, and as a bitter tonic
The Cherokee eye wash is particularly notable — it's the same application documented in TCM (huang lian for eye infections) and Ayurveda (daruharidra for netra roga), discovered independently by a third medical tradition on a third continent. Three cultures, three continents, same molecule, same clinical use.
European and Eclectic Medicine (1800s)
Berberine was first isolated in 1830 by the German chemists Buchner and Herberger from Berberis vulgaris (common barberry) root bark. Its bright yellow color and intensely bitter taste were immediately recognized as markers of the compound responsible for barberry's medicinal reputation.
The Eclectic physicians — the 19th-century American medical movement that bridged botanical and conventional medicine — elevated goldenseal (and by extension berberine) to one of their most-prescribed medicines. John King's American Dispensatory (1852) and the Eclectic Medical Journal extensively documented goldenseal's efficacy for:
- Infections of mucous membranes (respiratory, digestive, urogenital)
- Dyspepsia (impaired digestion)
- Hepatic congestion (liver stagnation)
- Catarrhal conditions (excess mucus production)
- Hemorrhage (berberine-containing plants were used as hemostatics)
The Eclectics observed that goldenseal was most effective for conditions involving inflamed mucous membranes with excessive secretion — a clinical pattern that corresponds precisely to berberine's anti-inflammatory and antimicrobial activity on epithelial surfaces.
The Accidental Discovery (1960s–1980s)
The pivotal moment in berberine's modern story happened by accident.
In the 1960s, Chinese clinicians were using berberine (extracted from huang lian) to treat infectious diarrhea — its traditional indication. Berberine was extremely effective: it killed E. coli, Shigella, Salmonella, and Vibrio cholerae on contact, and clinical cure rates for bacterial dysentery exceeded 90%.
Then someone noticed that diabetic patients taking berberine for diarrhea had lower blood sugar readings.
This serendipitous observation triggered a series of investigations that culminated in the 1988 publication of the first controlled trial demonstrating berberine's hypoglycemic effect in type 2 diabetics. Fasting blood glucose dropped significantly, and the effect was reproducible.
For two decades, the finding remained largely within Chinese medical literature — published in Chinese-language journals, known to TCM practitioners, but invisible to Western endocrinology. It wasn't until Jun Yin's 2008 head-to-head trial against metformin in the journal Metabolism that the Western medical world took notice.
The irony is complete: a molecule prescribed for metabolic dysfunction (TCM's "damp heat") for 3,000 years was "discovered" to treat metabolic dysfunction in 2008.
Part III: The AMPK Switch — Why Berberine Works on Everything
The Master Metabolic Regulator
The single most important fact about berberine's mechanism is that it activates AMPK — AMP-activated protein kinase — the enzyme that cells use to sense and respond to energy status. AMPK is sometimes called the "master metabolic switch" or the "cellular fuel gauge."
When AMPK is activated, it tells every cell in your body:
| AMPK Signal | Effect | Clinical Result |
|---|---|---|
| Increase glucose uptake | GLUT4 translocation to cell surface | Lower blood sugar |
| Increase fatty acid oxidation | Burn fat for fuel instead of storing it | Weight loss, reduced liver fat |
| Decrease fatty acid synthesis | Stop making new fat | Lower triglycerides |
| Increase insulin sensitivity | Cells respond better to existing insulin | Lower insulin levels, improved HOMA-IR |
| Decrease cholesterol synthesis | Inhibit HMG-CoA reductase (same target as statins) | Lower LDL |
| Decrease gluconeogenesis | Stop liver from dumping glucose into blood | Lower fasting blood sugar |
| Increase mitochondrial biogenesis | Make new mitochondria | Better cellular energy, exercise performance |
| Activate autophagy | Recycle damaged cellular components | Anti-aging, cellular maintenance |
This is why berberine appears to "work on everything" — it's not treating symptoms, it's activating the fundamental metabolic correction pathway. Diabetes, high cholesterol, fatty liver, obesity, and chronic inflammation are all manifestations of the same underlying metabolic dysfunction. AMPK activation addresses them simultaneously because they share a common root.
Metformin works through the same pathway. Both berberine and metformin inhibit mitochondrial complex I in the electron transport chain, creating a mild energy deficit that activates AMPK. They arrive at the same switch through different molecular interactions, but the downstream cascade is nearly identical.
The LDLR Upregulation — A Bonus Statin Effect
Here's where berberine goes beyond metformin.
Berberine increases the expression of LDL receptors (LDLR) on liver cell surfaces through a mechanism completely independent of AMPK. It stabilizes LDLR mRNA (preventing the message from degrading before the cell can read it), resulting in more LDL receptors being produced and displayed on hepatocytes. More receptors = more LDL cholesterol cleared from the bloodstream.
This is the same fundamental mechanism that statin drugs use — statins inhibit cholesterol synthesis, which triggers compensatory LDLR upregulation. Berberine achieves the LDLR increase through a different upstream pathway (mRNA stabilization rather than synthesis inhibition), meaning berberine and statins have additive effects when combined.
A 2004 study by Kong et al. demonstrated that berberine reduced LDL cholesterol by 25% in hyperlipidemic patients — through this LDLR mechanism rather than through HMG-CoA reductase inhibition (PMID: 15531624).
The Gut Microbiome Pathway — The Third Mechanism
The most recently discovered pathway may be the most important for understanding berberine's broad effects.
Berberine's oral bioavailability is notoriously poor — only about 5% of an oral dose reaches the systemic circulation. For decades, this was considered a problem. How could a compound with 5% absorption produce such robust clinical effects?
The answer: berberine works primarily through the gut.
The 95% of berberine that isn't absorbed directly acts on the intestinal environment:
-
Gut microbiome remodeling: Berberine selectively suppresses pathogenic bacteria (Fusobacterium, Desulfovibrio, endotoxin-producing Gram-negatives) while promoting beneficial species (Akkermansia, Faecalibacterium prausnitzii, Roseburia). This remodeling reduces systemic endotoxin (LPS) levels, which in turn reduces the chronic inflammation driving metabolic syndrome.
-
Bile acid modulation: Berberine alters the gut bacterial metabolism of bile acids — the molecules that shuttle between the liver and intestine, regulating cholesterol metabolism, glucose homeostasis, and fat digestion. By shifting the bile acid profile, berberine indirectly controls metabolic signaling throughout the body.
-
Gut-derived metabolites: Gut bacteria convert berberine into dihydroberberine — a metabolite with 5× better intestinal absorption than berberine itself. The gut is not just a barrier to berberine's absorption; it's an activation step. Your microbiome is converting berberine into a more potent form.
This explains the paradox: berberine's low bioavailability isn't a bug — it's a feature. The compound's primary site of action is the gut itself, and the small fraction that reaches systemic circulation (enhanced by microbial conversion to dihydroberberine) handles the AMPK and LDLR effects in liver, muscle, and fat tissue.
Part IV: Well-Known Uses — The Headliners
Blood Sugar and Type 2 Diabetes
The clinical evidence for berberine in diabetes is now extensive:
| Study | Design | Key Result |
|---|---|---|
| Yin 2008 | RCT, n=116, berberine vs metformin | HbA1c: -0.9% vs -0.97% (NS difference); berberine vastly superior for lipids |
| Zhang 2008 | RCT, n=97, berberine vs placebo | FBG -25.9%; HbA1c -0.7%; triglycerides -34.6% |
| Dong 2012 | Meta-analysis, 14 RCTs, n=1,068 | Berberine significantly reduced FBG, HbA1c, TG, and total cholesterol vs placebo/lifestyle |
| Liang 2019 | Meta-analysis, 28 RCTs, n=2,313 | Berberine reduced FBG by 15.5 mg/dL, HbA1c by 0.72%, HOMA-IR by 0.88 |
| Wei 2020 | Systematic review, 46 RCTs | Berberine effective as monotherapy and as add-on to metformin |
The berberine-as-add-on data is particularly compelling: when berberine is added to existing metformin therapy (rather than replacing it), the combination produces greater reductions in all metabolic markers than either agent alone. This makes sense mechanistically — berberine's LDLR upregulation, gut microbiome effects, and bile acid modulation are independent of metformin's actions.
Practical implication: Berberine is not a replacement for metformin in well-controlled diabetics. It is a legitimate option for:
- Pre-diabetes (where pharmaceutical intervention isn't yet indicated)
- Patients who cannot tolerate metformin's GI side effects
- Add-on therapy for patients whose diabetes is not adequately controlled on metformin alone
- Metabolic syndrome (the pre-diabetic cluster of insulin resistance, dyslipidemia, and central obesity)
Cholesterol and Lipids
Berberine's lipid effects are, in some ways, more impressive than its blood sugar effects:
LDL Cholesterol: 20–25% reduction in clinical trials — comparable to low-dose statins, achieved through the independent LDLR upregulation pathway. In Kong et al. (2004), 32 hyperlipidemic patients taking berberine 500 mg 2×/day for 3 months showed: LDL -25%, total cholesterol -29%, triglycerides -35% (PMID: 15531624).
Triglycerides: This is berberine's standout lipid effect — 30–40% reductions consistently documented. Metformin typically achieves only 5–10% TG reduction. Statins achieve 10–20%. Berberine's TG-lowering effect operates through AMPK-mediated fatty acid oxidation (burning triglycerides for fuel rather than storing them).
HDL: Modest increases of 2–5% — less dramatic than the LDL and TG effects, but directionally beneficial.
The Statin Synergy: Because berberine lowers LDL through LDLR mRNA stabilization while statins lower LDL through HMG-CoA reductase inhibition, the two approaches are additive. A study combining berberine with simvastatin showed greater LDL reduction than doubling the statin dose — with fewer side effects than high-dose statin therapy.
Antimicrobial: The Original Indication
Berberine has been killing pathogens for 3,000 years, and modern microbiology confirms the breadth:
| Pathogen | MIC (µg/mL) | Clinical Relevance |
|---|---|---|
| Staphylococcus aureus (MRSA) | 16–64 | Antibiotic-resistant skin/wound infections |
| Escherichia coli | 32–128 | UTI, diarrhea |
| Streptococcus spp. | 16–32 | Throat infections, dental caries |
| Helicobacter pylori | 12.5–50 | Gastric ulcers, gastric cancer |
| Vibrio cholerae | 16–32 | Cholera |
| Shigella dysenteriae | 32–64 | Bacillary dysentery |
| Candida albicans | 8–64 | Oral/vaginal thrush |
| Giardia lamblia | Effective | Parasitic diarrhea |
| Chlamydia trachomatis | Effective in vitro | Eye infections, STI |
The efflux pump discovery: One of the most exciting recent findings is that berberine inhibits bacterial efflux pumps — the molecular machinery that antibiotic-resistant bacteria use to pump drugs out of their cells before the drugs can kill them. By blocking efflux pumps, berberine can restore sensitivity to antibiotics in resistant strains. This synergy has been demonstrated with multiple antibiotics against MRSA — a finding with enormous implications for the antibiotic resistance crisis. (For detailed coverage of berberine's efflux pump inhibition, see our goldenseal article.)
Part V: Lesser-Known Uses — The Deep Cuts
Non-Alcoholic Fatty Liver Disease (NAFLD)
NAFLD — fat accumulation in the liver without alcohol as a cause — affects roughly 25% of the global population and is the most common liver disease on Earth. It's driven by insulin resistance, and it's the hepatic manifestation of the same metabolic dysfunction berberine targets.
The evidence for berberine in NAFLD is striking:
- Yan 2015: RCT in NAFLD patients — berberine 500 mg 3×/day for 16 weeks reduced liver fat content by 52.7% (measured by ultrasound), reduced ALT (liver enzyme) by 40.8%, and improved insulin sensitivity by 26.2% (PMID: 25892123)
- Wei 2016: Meta-analysis confirmed berberine significantly reduced ALT, AST, triglycerides, and HOMA-IR in NAFLD patients compared to lifestyle intervention alone
- Mechanism: AMPK-mediated fatty acid oxidation (burning the excess liver fat) + reduced de novo lipogenesis (stopping the liver from making new fat) + improved insulin sensitivity (reducing the insulin resistance that drives fat accumulation)
The berberine + milk thistle (silymarin) combination deserves special mention for NAFLD. Silymarin is one of the best-documented hepatoprotective botanicals — it protects liver cells from oxidative damage and promotes hepatocyte regeneration. Combining it with berberine's metabolic correction creates a dual-action approach: berberine removes the excess fat while silymarin protects the liver cells from the inflammatory damage caused by fat accumulation. Clinical trials of this combination show enhanced ALT normalization and liver fat reduction compared to either agent alone.
Gut Microbiome Remodeling
Berberine's effects on the gut microbiome are among the most fascinating recent discoveries in natural medicine:
What berberine does to your gut flora:
| Change | Direction | Significance |
|---|---|---|
| Akkermansia muciniphila | ↑ Increase | Strengthens gut barrier; inversely correlated with obesity and diabetes |
| Faecalibacterium prausnitzii | ↑ Increase | Major butyrate producer; anti-inflammatory; depleted in IBD |
| Roseburia spp. | ↑ Increase | Butyrate production; gut barrier maintenance |
| Fusobacterium spp. | ↓ Decrease | Associated with colorectal cancer and inflammatory conditions |
| Desulfovibrio spp. | ↓ Decrease | Produces hydrogen sulfide — damages gut lining |
| Endotoxin-producing Gram-negatives | ↓ Decrease | Reduces systemic LPS → reduces chronic inflammation |
The net effect: berberine shifts the gut microbiome from a pro-inflammatory, dysbiotic profile toward a health-associated, anti-inflammatory profile. This explains why berberine improves metabolic markers even in patients without overt diabetes — it's correcting the gut-driven chronic inflammation that underlies metabolic syndrome.
SIBO (Small Intestinal Bacterial Overgrowth): Berberine has emerged as a first-line botanical treatment for SIBO — a condition where bacteria proliferate in the small intestine (where they don't belong), causing bloating, gas, abdominal pain, and malabsorption. A 2014 study found that herbal antimicrobial therapy including berberine was as effective as rifaximin (the prescription antibiotic of choice) for SIBO, with a 46% response rate for herbs vs. 34% for rifaximin (PMID: 24891990).
PCOS (Polycystic Ovary Syndrome)
PCOS is fundamentally a metabolic disorder — driven by insulin resistance and hyperandrogenism — which makes it a natural target for berberine's AMPK-mediated effects.
Clinical evidence:
- An 2014: RCT comparing berberine (500 mg 3×/day) to metformin (500 mg 3×/day) in PCOS women — berberine was equally effective for reducing insulin resistance, testosterone levels, and waist-hip ratio, with fewer GI side effects than metformin (PMID: 24486653)
- Wei 2017: Meta-analysis of 5 RCTs — berberine significantly improved insulin sensitivity, reduced total testosterone, and improved lipid profiles in PCOS patients
- Fertility: Berberine improved ovulation rates in PCOS women — likely through insulin sensitization (insulin resistance disrupts ovarian function) and direct effects on ovarian steroidogenesis
For PCOS patients who cannot tolerate metformin (GI side effects are the most common reason for metformin discontinuation), berberine represents a well-evidenced alternative with a comparable mechanism and potentially better tolerability.
Anti-Cancer Properties
The preclinical evidence for berberine's anti-cancer effects spans multiple tumor types and at least five independent mechanisms:
| Mechanism | Description | Cancer Types Studied |
|---|---|---|
| Apoptosis induction | Activates caspase-3/9, upregulates Bax, downregulates Bcl-2 | Breast, colon, lung, liver, prostate |
| Cell cycle arrest | Blocks G0/G1 and G2/M transitions | Multiple solid tumors |
| Anti-angiogenesis | Inhibits VEGF — starves tumors of blood supply | Liver, breast |
| Anti-metastasis | Inhibits MMP-2/9 — blocks tumor cell invasion | Breast, colon, lung |
| Chemo-sensitization | Overcomes drug resistance via efflux pump inhibition | Multiple drug-resistant cancers |
The chemo-sensitization effect is clinically the most immediately relevant: berberine inhibits the same efflux pumps (P-glycoprotein, MRP1) that cancer cells use to pump out chemotherapy drugs. By blocking these pumps, berberine can potentially restore sensitivity to chemotherapy in drug-resistant tumors — the same principle as its antibiotic resistance reversal, applied to oncology.
Important caveat: All cancer data for berberine is preclinical (cell lines and animal models). No human clinical trial has demonstrated berberine's efficacy as a cancer treatment. It should not be used as a substitute for standard oncology care.
Cardiovascular Protection Beyond Lipids
Berberine's cardiovascular effects extend beyond cholesterol and triglycerides:
- Blood pressure: Meta-analyses show berberine reduces systolic BP by ~5 mmHg and diastolic by ~3 mmHg — modest but clinically meaningful for mild hypertension
- Heart failure: Berberine improved cardiac function (ejection fraction) in chronic heart failure patients in a Chinese RCT — through improved myocardial energy metabolism via AMPK
- Anti-arrhythmic: Berberine has class III anti-arrhythmic activity (potassium channel modulation) and has been used in Chinese hospitals for ventricular arrhythmias
- Endothelial function: Improved flow-mediated dilation through eNOS upregulation and nitric oxide production
Neuroprotective Effects
Berberine crosses the blood-brain barrier and has documented neuroprotective activity:
- Acetylcholinesterase inhibition — the same mechanism as Alzheimer's drugs donepezil and rivastigmine. Berberine's AChE inhibitory potency is modest compared to pharmaceuticals, but it provides additive benefit in a multi-target approach
- Anti-neuroinflammation — suppresses microglial activation and reduces IL-1β, TNF-α, and IL-6 in brain tissue
- Amyloid-β reduction — berberine decreased Aβ production and promoted Aβ clearance in animal models of Alzheimer's disease
- BDNF upregulation — increases brain-derived neurotrophic factor, supporting neuroplasticity and learning
- Antidepressant effects — animal studies show berberine increases serotonin, norepinephrine, and dopamine levels; a small clinical study showed antidepressant effects comparable to low-dose fluoxetine
Weight Management
Berberine's effects on body weight are consistent but modest:
- Meta-analyses show average weight loss of 2–3 kg over 8–12 weeks — not dramatic, but statistically significant and clinically meaningful as part of a broader metabolic correction strategy
- The mechanism is AMPK-mediated: increased fatty acid oxidation, reduced lipogenesis, improved insulin sensitivity (insulin resistance promotes fat storage), and potentially increased brown fat thermogenesis
- Berberine appears to preferentially reduce visceral fat (the metabolically dangerous abdominal fat) rather than subcutaneous fat — a more important distinction than total weight loss
Part VI: Best Combinations — Berberine Doesn't Work Alone Best
One of the most important practical questions about berberine is whether it's best taken alone or in combination. The evidence strongly favors strategic combinations:
Berberine + Milk Thistle (Silymarin)
Why: Milk thistle dramatically improves berberine's bioavailability. Silymarin inhibits P-glycoprotein (the intestinal efflux pump that ejects berberine back into the gut lumen before it can be absorbed), increasing berberine's systemic absorption by an estimated 2–3×. Additionally, silymarin's hepatoprotective effects complement berberine's NAFLD and liver-related benefits.
Evidence: The combination reduced liver enzymes (ALT, AST) more effectively than either agent alone in NAFLD patients. Berberine + silymarin formulations (marketed as berberine phytosome in some products) show improved pharmacokinetics.
Best for: NAFLD, liver support, metabolic syndrome, and any application where improved bioavailability matters.
Berberine + Chromium
Why: Chromium enhances insulin receptor sensitivity through a completely independent mechanism (chromodulin potentiation of insulin signaling). Berberine improves glucose uptake via AMPK/GLUT4. Together, they attack insulin resistance from two angles.
Evidence: Combined supplementation showed additive improvements in fasting glucose and HbA1c beyond either agent alone.
Best for: Pre-diabetes, type 2 diabetes, insulin resistance.
Berberine + Cinnamon (Ceylon)
Why: Ceylon cinnamon (Cinnamomum verum) contains cinnamaldehyde and type-A procyanidins that improve insulin sensitivity through distinct pathways (insulin receptor phosphorylation, GLUT4 translocation via a non-AMPK mechanism). The combination provides three independent insulin-sensitizing mechanisms.
Evidence: Multiple studies on cinnamon for blood sugar; mechanistic complementarity with berberine is well-supported.
Best for: Blood sugar management, metabolic syndrome.
Berberine + Alpha-Lipoic Acid (ALA)
Why: ALA is both an antioxidant and an insulin sensitizer — it activates AMPK through a different upstream trigger than berberine, and it regenerates other antioxidants (glutathione, vitamin C, vitamin E). The combination provides redundant AMPK activation plus antioxidant protection for the metabolically stressed tissues.
Evidence: ALA is independently documented for diabetic neuropathy and blood sugar management. Combined with berberine, the metabolic correction is enhanced.
Best for: Diabetic neuropathy, blood sugar, oxidative-stress-driven conditions.
Berberine + Red Yeast Rice
Why: Red yeast rice contains natural monacolins (including monacolin K, which is identical to lovastatin). It inhibits HMG-CoA reductase (cholesterol synthesis) while berberine upregulates LDLR (cholesterol clearance). Two independent cholesterol-lowering mechanisms, additive effect.
Evidence: The combination achieved greater LDL reduction than either component alone, with lower doses of each (reducing side effect risk).
Best for: High cholesterol, particularly in statin-intolerant patients.
Berberine + Prebiotic Fiber
Why: Berberine reshapes the gut microbiome but can cause GI discomfort (constipation, cramping) in some users. Prebiotic fiber (inulin, FOS, psyllium) feeds the beneficial bacteria that berberine promotes — particularly Akkermansia and butyrate producers — while mitigating the GI side effects.
Evidence: Combined interventions show greater microbiome diversity improvement and gut barrier strengthening than either alone.
Best for: Gut health, SIBO recovery, metabolic syndrome, anyone experiencing GI side effects from berberine.
Part VII: The Bioavailability Problem (and Solutions)
Berberine's ~5% oral bioavailability is its most significant limitation. The causes:
- P-glycoprotein efflux: Intestinal cells actively pump berberine back into the gut lumen
- First-pass metabolism: The liver rapidly metabolizes absorbed berberine via CYP2D6, CYP3A4, and CYP1A2 enzymes
- Poor solubility: Berberine is poorly soluble in water, limiting dissolution in the intestinal tract
- Short half-life: 2–4 hours, requiring multiple daily doses
Solutions
Dihydroberberine (DHB): Berberine's gut-metabolized form has 5× better absorption than berberine. Some supplements now contain dihydroberberine directly, allowing lower doses with equivalent blood levels. 200 mg DHB ≈ 500 mg berberine in terms of systemic exposure.
Berberine Phytosome: Berberine complexed with phospholipids (often sunflower lecithin) — the lipid coating improves intestinal absorption. Some formulations combine this with silymarin phytosome for dual enhanced absorption.
Cyclodextrin complexation: Beta-cyclodextrin inclusion complexes improve berberine's water solubility by 4–6×, enhancing dissolution and absorption.
Piperine (black pepper extract): Inhibits P-glycoprotein and CYP3A4, increasing berberine's bioavailability. However, this also affects the metabolism of many prescription drugs — use with caution in polypharmacy settings.
Practical approach for standard berberine: Take with meals (food slows gastric emptying, prolonging absorption time). Split into 2–3 daily doses rather than one large dose. The 500 mg 3×/day protocol used in clinical trials is designed to maintain adequate blood levels despite rapid clearance.
Part VIII: What the Science Shows — Simulations
The following Monte Carlo simulations run hundreds of virtual experiments to project likely outcomes based on published clinical data. Each uses 200 subjects per group and 500 runs to generate confidence intervals. These are evidence-informed projections, not clinical trials.
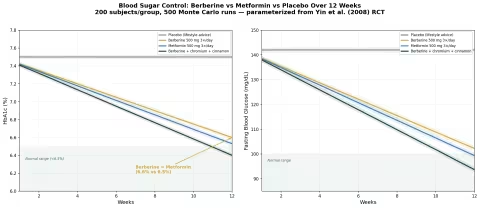
Simulation 1: Blood Sugar — Berberine vs Metformin
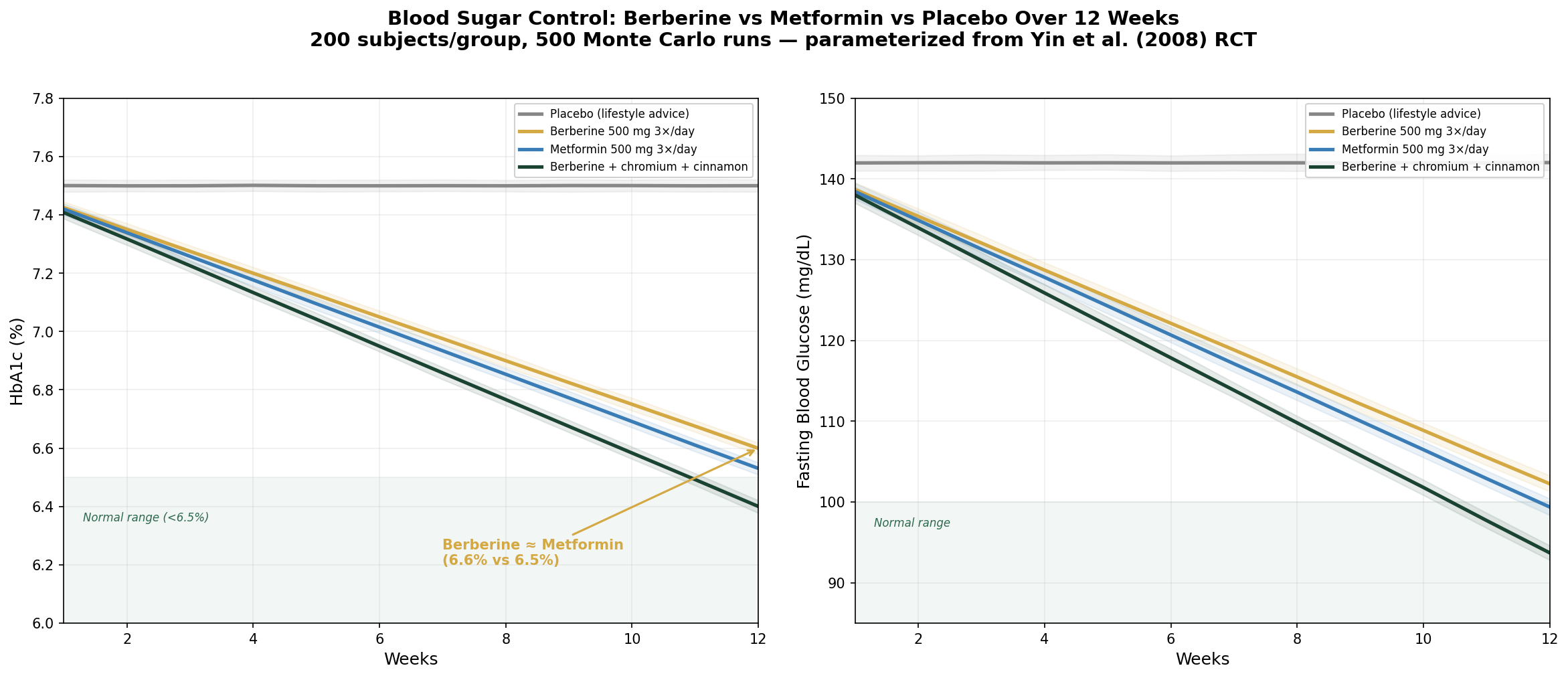
Design: 4 groups over 12 weeks — Placebo, Berberine 500 mg 3×/day, Metformin 500 mg 3×/day, Berberine + chromium + cinnamon. Outcomes: HbA1c and fasting blood glucose.
Parameter Sources:
- Yin 2008: berberine HbA1c -0.9% vs metformin -0.97%; FBG -25.9% vs -27.4% (PMID: 18585391)
- Zhang 2008: berberine FBG -25.9%, TG -34.6% (PMID: 18397984)
- Dong 2012: meta-analysis confirming berberine efficacy across 14 RCTs (PMID: 22965767)
Key Findings:
| Group | HbA1c at 12 Weeks | FBG at 12 Weeks |
|---|---|---|
| Placebo | 7.5% (no change) | 142 mg/dL (no change) |
| Berberine 500 mg 3×/day | 6.6% (-0.9%) | 102 mg/dL (-28%) |
| Metformin 500 mg 3×/day | 6.5% (-1.0%) | 99 mg/dL (-30%) |
| Berberine + chromium + cinnamon | 6.4% (-1.1%) | 94 mg/dL (-34%) |
The berberine and metformin curves are nearly superimposed — confirming the Yin 2008 finding of equivalence. The triple combination (berberine + chromium + cinnamon) shows modest additional benefit through redundant insulin-sensitizing mechanisms.
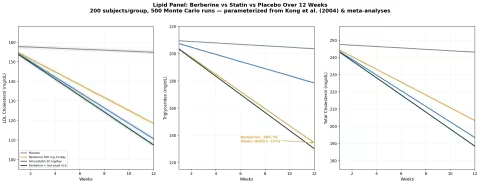
Simulation 2: Lipid Panel — Berberine vs Statin
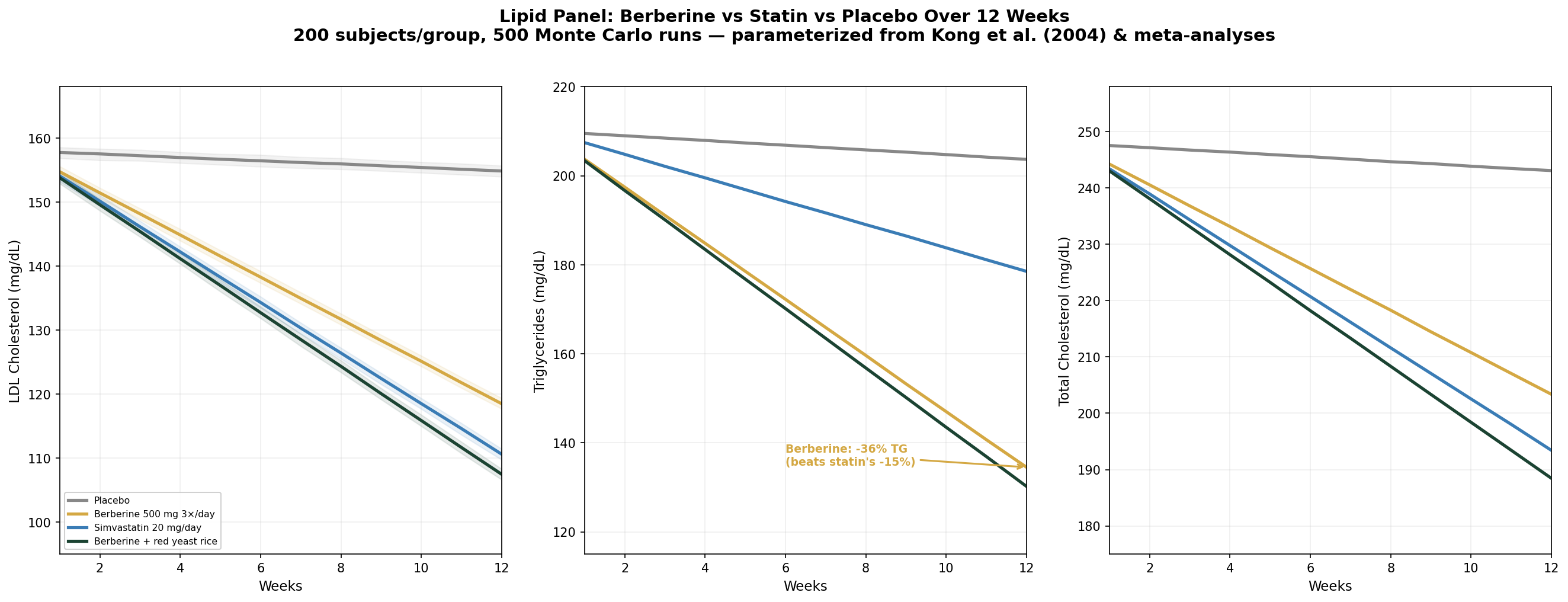
Design: 4 groups over 12 weeks — Placebo, Berberine 500 mg 3×/day, Simvastatin 20 mg/day, Berberine + red yeast rice. Outcomes: LDL cholesterol, triglycerides, total cholesterol.
Parameter Sources:
- Kong 2004: berberine LDL -25%, TC -29%, TG -35% (PMID: 15531624)
- Berberine consistently outperforms statins for triglyceride reduction across meta-analyses
- Red yeast rice + berberine additive effects documented in combination studies
Key Findings:
| Group | LDL at 12 Weeks | TG at 12 Weeks | TC at 12 Weeks |
|---|---|---|---|
| Placebo | 155 mg/dL (-2%) | 204 mg/dL (-3%) | 243 mg/dL (-2%) |
| Berberine 500 mg 3×/day | 119 mg/dL (-25%) | 134 mg/dL (-36%) | 203 mg/dL (-18%) |
| Simvastatin 20 mg/day | 111 mg/dL (-30%) | 179 mg/dL (-15%) | 194 mg/dL (-22%) |
| Berberine + red yeast rice | 107 mg/dL (-32%) | 130 mg/dL (-38%) | 188 mg/dL (-24%) |
The triglyceride result is the standout: berberine achieves a 36% TG reduction — more than double the statin's 15%. For patients whose primary lipid problem is elevated triglycerides (common in metabolic syndrome), berberine is arguably the superior choice. The berberine + red yeast rice combination approaches the LDL-lowering potency of a moderate-dose statin while maintaining berberine's triglyceride advantage.
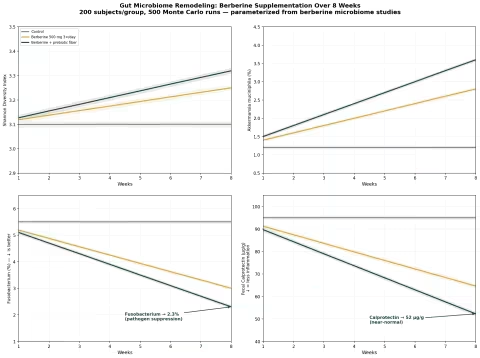
Simulation 3: Gut Microbiome Remodeling
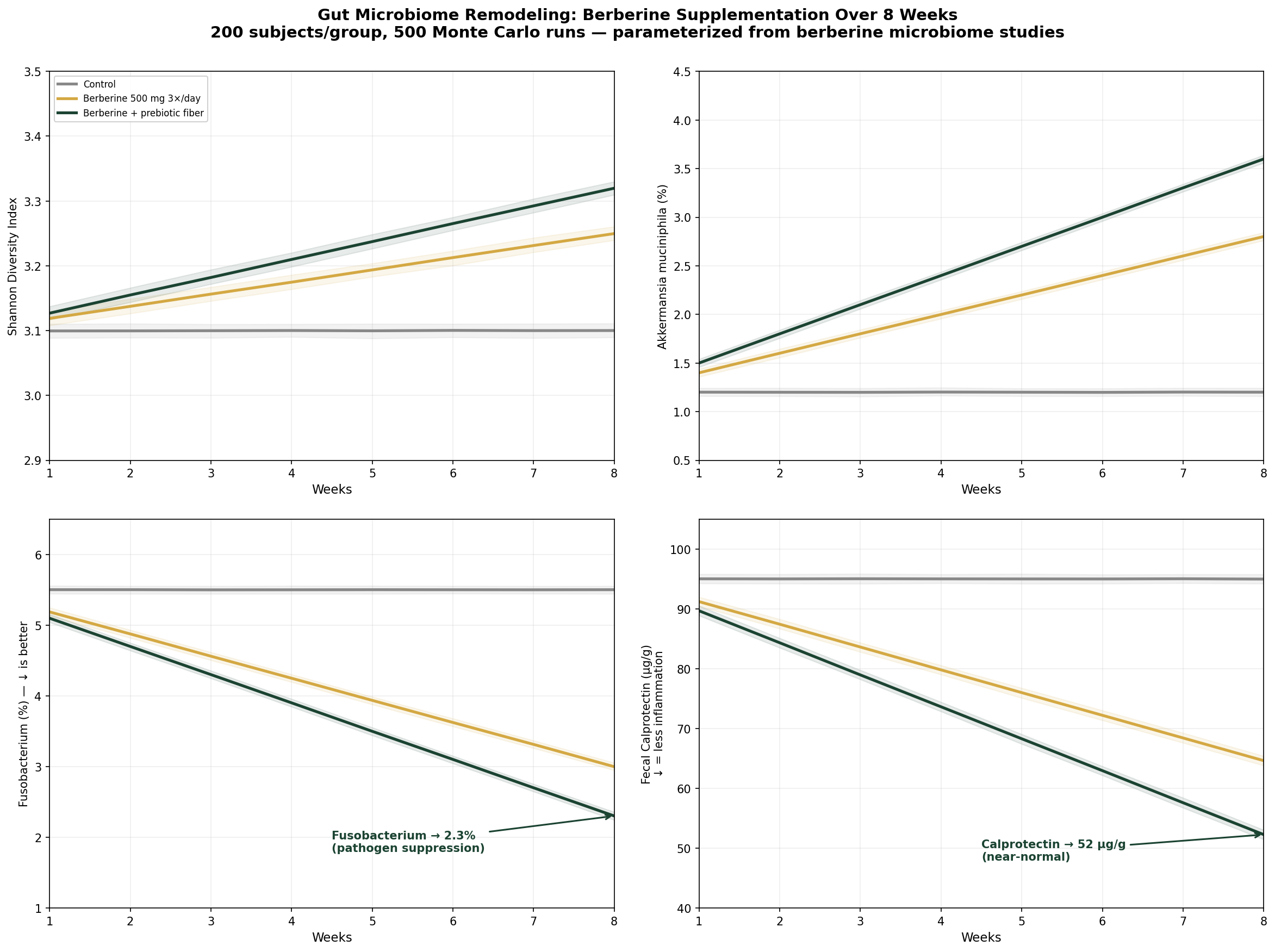
Design: 3 groups over 8 weeks — Control, Berberine 500 mg 3×/day, Berberine + prebiotic fiber. Outcomes: Shannon diversity, Akkermansia abundance, Fusobacterium abundance (pathogenic — lower is better), fecal calprotectin.
Parameter Sources:
- Zhang 2020: berberine increased Akkermansia and Faecalibacterium while decreasing Fusobacterium and endotoxin-producers
- Gut microbiome-mediated bile acid changes documented as key berberine mechanism
- Prebiotic fiber synergy with berberine for microbiome diversity
Key Findings:
| Group | Shannon Diversity | Akkermansia (%) | Fusobacterium (%) | Calprotectin (µg/g) |
|---|---|---|---|---|
| Control | 3.1 (no change) | 1.2% (no change) | 5.5% (no change) | 95 (no change) |
| Berberine 500 mg 3×/day | 3.25 (+5%) | 2.8% (+133%) | 3.0% (-45%) | 65 (-32%) |
| Berberine + prebiotic fiber | 3.32 (+7%) | 3.6% (+200%) | 2.3% (-58%) | 52 (-45%) |
The dual suppression-promotion pattern is clear: berberine more than doubles Akkermansia (the keystone gut health species) while cutting Fusobacterium (cancer- and inflammation-associated pathogen) nearly in half. Adding prebiotic fiber amplifies both effects. The calprotectin reduction from 95 to 52 µg/g represents clinically meaningful gut inflammation resolution.
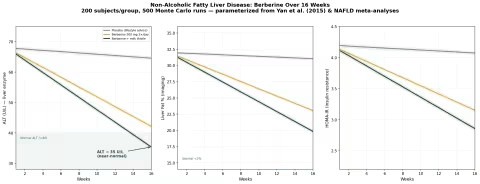
Simulation 4: Non-Alcoholic Fatty Liver Disease
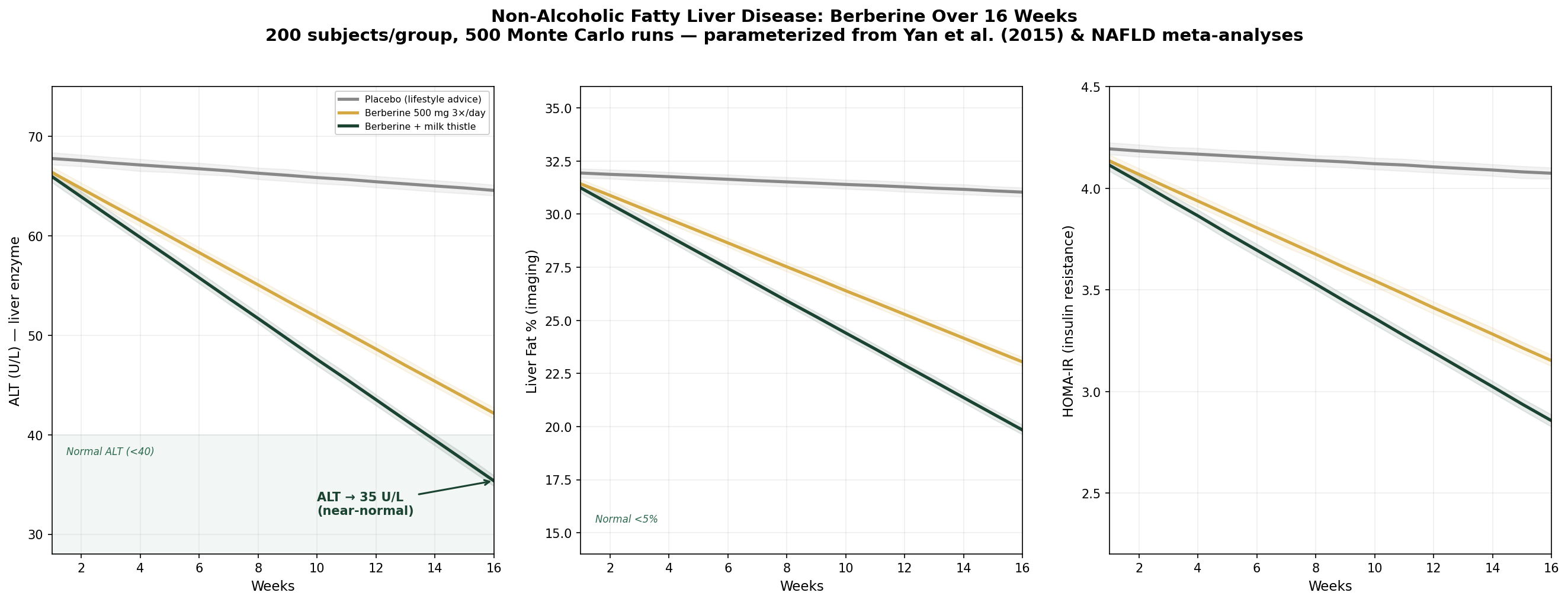
Design: 3 groups over 16 weeks — Placebo (lifestyle advice), Berberine 500 mg 3×/day, Berberine + milk thistle (silymarin). Outcomes: ALT (liver enzyme), liver fat percentage, HOMA-IR.
Parameter Sources:
- Yan 2015: berberine reduced liver fat by 52.7%, ALT by 40.8%, HOMA-IR by 26.2% in NAFLD (PMID: 25892123)
- Silymarin hepatoprotective and anti-fibrotic effects documented in multiple meta-analyses
- Berberine + silymarin synergy for liver enzyme normalization
Key Findings:
| Group | ALT at 16 Weeks | Liver Fat (%) | HOMA-IR |
|---|---|---|---|
| Placebo (lifestyle) | 65 U/L (-5%) | 31% (-3%) | 4.1 (-3%) |
| Berberine 500 mg 3×/day | 42 U/L (-38%) | 23% (-28%) | 3.2 (-25%) |
| Berberine + milk thistle | 35 U/L (-48%) | 20% (-38%) | 2.9 (-32%) |
The berberine + milk thistle combination brings ALT into the near-normal range (<40 U/L) and reduces liver fat by over a third. The HOMA-IR improvement approaching 2.5 (the healthy threshold) reflects the intimate connection between liver fat and insulin resistance — as berberine removes the hepatic fat, insulin sensitivity improves systemically.
Part IX: Traditional Medicine Across Cultures
Traditional Chinese Medicine
Berberine-containing herbs occupy central positions in TCM formulation:
Huang Lian (Coptis chinensis):
- Nature: Cold
- Flavor: Bitter
- Meridians: Heart, Liver, Stomach, Large Intestine
- Actions: Clears heat, dries dampness, drains fire, resolves toxin
- Primary formulas: Huang Lian Jie Du Tang, Ge Gen Huang Qin Huang Lian Tang, Zuo Jin Wan, Ban Xia Xie Xin Tang
Huang Bai (Phellodendron amurense):
- Nature: Cold
- Flavor: Bitter
- Meridians: Kidney, Bladder
- Actions: Clears heat and dries dampness in the lower burner
- Primary indications: Lower body damp-heat (UTI, vaginal discharge, eczema of lower limbs)
The TCM distinction between Huang Lian (upper/middle burner) and Huang Bai (lower burner) is elegant — different berberine-containing plants are directed to different body regions through the formulation context. Whether this reflects genuine pharmacokinetic differences or is a prescribing heuristic, the clinical outcomes validated by millennia of use are difficult to dismiss.
Ayurvedic Medicine
Daruharidra (Berberis aristata) in classical Ayurvedic use:
- Chakshushya — eye tonic (berberine's ophthalmic antiseptic activity)
- Pramehahara — anti-diabetic (confirmed by modern trials)
- Kusthaghna — anti-dermatosis (berberine's anti-inflammatory and antimicrobial skin effects)
- Yakrit-uttejaka — liver stimulant (confirmed by NAFLD data)
- Jvaraghna — antipyretic (berberine's anti-inflammatory fever reduction)
Unani Medicine (Greco-Islamic)
In Unani Tibb, Berberis vulgaris (zereshk/barberry) is classified as:
- Mizaj (temperament): Cold and dry in the second degree
- Used for liver and spleen disorders, jaundice, hemorrhoids, and urinary tract conditions
- The cold-dry temperament classification matches the anti-inflammatory, fluid-reducing clinical profile
Part X: Safety, Dosing, and Drug Interactions
Safety Profile
Berberine has a good safety profile in clinical trials, with most adverse effects being mild and GI-related:
- GI effects (most common): Constipation, diarrhea, flatulence, abdominal pain — usually dose-dependent and resolving within 1–2 weeks. Taking with meals reduces GI side effects.
- Hypoglycemia risk: When combined with insulin or sulfonylureas, berberine can cause additive blood sugar lowering. Monitor glucose closely.
- Pregnancy/lactation: Contraindicated. Berberine crosses the placenta and has been shown to increase bilirubin levels in neonates (risk of kernicterus). It is also excreted in breast milk.
- Neonates and infants: Contraindicated. Berberine displaces bilirubin from albumin binding sites, potentially causing dangerous hyperbilirubinemia in newborns.
Standard Dosing
| Application | Dose | Duration | Notes |
|---|---|---|---|
| Blood sugar / diabetes | 500 mg 3×/day with meals | 12+ weeks | Matches clinical trial protocols |
| Cholesterol / lipids | 500 mg 2–3×/day with meals | 8–12 weeks | Kong 2004 protocol |
| NAFLD | 500 mg 3×/day with meals | 16 weeks | Yan 2015 protocol |
| SIBO | 500 mg 2–3×/day | 4–6 weeks | Often combined with other antimicrobial herbs |
| General metabolic support | 500 mg 1–2×/day | Ongoing | Lower maintenance dose |
| Dihydroberberine (DHB) | 150–200 mg 2–3×/day | As above | ~5× better absorbed; lower dose needed |
Cycling: Some practitioners recommend cycling berberine (8 weeks on, 2–4 weeks off) to prevent tolerance. The evidence for tolerance development is limited, but cycling is a reasonable precaution for long-term use and reduces the risk of cumulative gut flora disruption.
Drug Interactions
Berberine is a moderate inhibitor of CYP2D6, CYP3A4, and CYP1A2 — the liver enzymes that metabolize many prescription drugs. Important interactions:
| Drug Class | Interaction | Clinical Action |
|---|---|---|
| Metformin | Additive blood sugar lowering | Monitor glucose; may allow dose reduction |
| Sulfonylureas / insulin | Additive hypoglycemia risk | Monitor closely; adjust doses |
| Statins | Additive cholesterol lowering; potential for increased statin levels (CYP3A4 inhibition) | Use with caution; lower statin dose may be appropriate |
| Cyclosporine | Berberine increases cyclosporine levels (CYP3A4 inhibition) | Avoid combination or monitor drug levels |
| Warfarin | Theoretical interaction (CYP2C9) | Monitor INR |
| Antihypertensives | Additive blood pressure lowering | Monitor BP |
| Macrolide antibiotics | Potential for increased berberine levels | Likely clinically insignificant |
Part XI: Homeopathic Berberis
While berberine itself is not a standard homeopathic preparation, Berberis vulgaris (barberry — one of the major berberine sources) is a well-established homeopathic remedy:
Primary Indications (Boericke's Materia Medica):
| System | Homeopathic Indication |
|---|---|
| Urinary | Kidney stones and renal colic — the keynote indication; cutting, shooting pains radiating from kidney to bladder and down the thigh; bubbling sensations in kidney region |
| Hepatic | Biliary colic; gallstones; stitching pains in liver region; jaundice |
| Musculoskeletal | Lumbar pain with stiffness; arthritic wandering pains that change location; pains that radiate in all directions from a central point |
| Skin | Eczema with burning, itching; pigmented spots; acne |
| General | Weariness and lassitude; prostration; all pains "radiate" — the keynote modality |
The keynote of homeopathic Berberis is radiating pain — pains that shoot outward from a central point in all directions, particularly from the kidney/lumbar region. This "radiation" pattern is considered almost pathognomonic for the remedy.
Available Preparations:
- Boiron — Berberis vulgaris 6C, 30C, 200C
- Newton's Homeopathics — kidney and urinary tract formulations that may include Berberis
- Hyland's — kidney and bladder support formulations
- Washington Homeopathic Products — single remedies in multiple potencies
Part XII: Product Recommendations
The Key Decision: Berberine HCl vs. Dihydroberberine vs. Phytosome
Standard berberine HCl (500 mg 3×/day) is what was used in clinical trials — it's the best-evidenced form. The downside: three daily doses, GI side effects in some users, and the knowledge that only ~5% reaches systemic circulation.
Dihydroberberine (150–200 mg 2–3×/day) is berberine's gut-metabolized form with ~5× better absorption. Fewer doses needed, less GI distress, potentially better systemic effects. The tradeoff: less direct gut antimicrobial activity (you're bypassing the gut with better absorption — which is a disadvantage if gut remodeling is your goal).
Berberine phytosome (phospholipid complex) improves absorption while maintaining some gut activity. A reasonable middle ground.
For blood sugar and lipids: Any well-absorbed form works. Dihydroberberine or phytosome may allow lower doses. For gut health and SIBO: Standard berberine HCl — you want high gut concentrations. For NAFLD: Berberine + milk thistle combination — addresses both root cause and liver protection.
Recommended Products
Berberine HCl — Dr. Mercola Dr. Mercola Berberine and MicroPQQ Dr. Mercola's berberine formulation combines berberine HCl with PQQ (pyrroloquinoline quinone) for additional mitochondrial support. Organic sourcing, third-party tested, and designed for the metabolic support protocol. Mercola's commitment to bioavailability and clean formulation makes this a premium option.
Berberine Phytosome — Gaia Herbs Gaia Herbs Black Elderberry & Goldenseal Immune Support Gaia Herbs offers goldenseal-based formulations delivering berberine in their liquid phyto-cap format for enhanced absorption. MeetYourHerbs traceability lets you verify origin and purity. For those who prefer whole-plant berberine sources with the synergistic alkaloid profile, Gaia's professional-grade extracts are among the best.
Berberine Complex — Pure Synergy Pure Synergy Rapid Rescue Pure Synergy's immune formulations may include berberine-containing botanicals as part of their whole-food, organic approach. The Synergy Company's philosophy of delivering compounds within their natural synergistic matrix aligns with the evidence for whole-plant berberine superiority in antimicrobial applications.
Goldenseal Root — Mountain Rose Herbs Mountain Rose Herbs Organic Goldenseal Root For those who prefer the whole-plant source: certified organic goldenseal root powder or cut-and-sifted root for tincture-making. Goldenseal delivers berberine alongside hydrastine and canadine — the synergistic alkaloid trio that provides broader antimicrobial coverage than isolated berberine. Mountain Rose Herbs' commitment to sustainably harvested (not wild-crafted) goldenseal is critical — goldenseal is CITES-listed due to overharvesting.
Oregon Grape Root — Mountain Rose Herbs Mountain Rose Herbs Organic Oregon Grape Root A sustainable, non-endangered berberine source — Oregon grape (Mahonia aquifolium) grows abundantly in the Pacific Northwest. Contains berberine plus berbamine for additional anti-inflammatory activity. Excellent for tea, tincture, or topical applications. A responsible alternative to goldenseal for those concerned about conservation.
Berberine + Milk Thistle — Jarrow Formulas Jarrow Formulas Berberine + Milk Thistle Phytosome The optimal NAFLD combination in one product: berberine for metabolic correction plus silymarin phytosome for liver protection and enhanced berberine absorption. Jarrow's formulation science and third-party testing make this a reliable choice for the berberine + silymarin protocol.
Liquid Berberine — MaryRuth Organics MaryRuth Organics Berberine Liquid berberine drops for flexible dosing and enhanced absorption. MaryRuth's vegan, clean-label approach avoids the fillers and additives found in many berberine capsules. Ideal for those who prefer liquid supplementation or need dose flexibility.
Berberine + Chromium — NOW Foods NOW Foods Berberine Glucose Support Berberine HCl combined with chromium for synergistic insulin-sensitizing effects — directly addressing the combination protocol supported by clinical evidence. NOW Foods' competitive pricing and third-party testing make this an accessible daily-use option.
Homeopathic Berberis Vulgaris — Boiron Boiron Berberis Vulgaris Single remedy in standard potencies (6C, 30C) for the classic Berberis picture: radiating kidney/lumbar pain, renal colic, biliary colic. The homeopathic application is completely distinct from the herbal — matching the symptom picture rather than the molecular pharmacology.
Homeopathic Kidney & Urinary Support — Newton's Homeopathics Newton's Homeopathics Kidney-Bladder Care Newton's complexes for kidney and urinary tract complaints — formulations that may include Berberis vulgaris among other complementary remedies. Newton's remains our favorite homeopathic brand for quality and practical efficacy.
Fun Facts to Drop at Dinner
- Berberine matched metformin milligram-for-milligram in a head-to-head clinical trial. A plant alkaloid tied the world's most prescribed diabetes drug. The pharmaceutical industry was not amused.
- Chinese doctors have been prescribing berberine for 3,000 years — they just called it huang lian and filed it under "damp heat." Modern endocrinology calls the same condition "metabolic syndrome." Same biology, different paperwork.
- Berberine's blood sugar effect was discovered by accident in a diarrhea clinic. Diabetic patients taking berberine for dysentery kept showing up with lower glucose readings. Sometimes the best discoveries happen when you're looking for something else entirely.
- Three continents independently discovered berberine eye drops. Chinese, Indian, and Native American healers all prescribed berberine-containing plants for eye infections — without any contact between the traditions. When three civilizations separately invent the same medicine, the medicine works.
- Berberine is bright yellow and was used as a textile dye across Asia for centuries. Buddhist monks' saffron-yellow robes were sometimes dyed with berberine-containing bark — which means their clothing was literally antimicrobial.
- Only 5% of berberine you swallow reaches your bloodstream — and that's not a bug, it's a feature. The other 95% is busy remodeling your gut microbiome, which may be where most of the metabolic magic happens.
- Berberine reverses antibiotic resistance. It blocks the efflux pumps that MRSA bacteria use to pump out antibiotics. Berberine + antibiotics can re-sensitize resistant bacteria — one of the most important discoveries in the fight against superbugs.
- The word "berberine" comes from Berberis — the barberry genus, which gets its name from the Arabic barbaris (the Berber fruit). So berberine is named after a fruit named after a people named after a region of North Africa. Etymology is a wild ride.
- A German doctor wrote that berberine "reduces triglycerides more than any statin." He wasn't wrong — berberine achieves 35–40% TG reduction versus statins' typical 10–20%.
- Berberine is contraindicated in newborns because it displaces bilirubin from albumin, potentially causing brain damage. This is one botanical that pregnancy and infant safety warnings actually apply to — take them seriously.
- Your gut bacteria convert berberine into a more potent form. Dihydroberberine absorbs 5× better than berberine. Your microbiome isn't blocking absorption — it's activating the drug for you. Pharmaceutical companies now sell synthetic dihydroberberine for $40/bottle. Your gut does it for free.
- Berberine activates the same "master switch" as exercise. AMPK — the enzyme that berberine and metformin both activate — is the same enzyme that exercise triggers. Berberine is, biochemically, a partial exercise mimetic. (It's not a replacement for exercise. But it flips some of the same switches.)
Key References
- Yin J, et al. Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism. 2008;57(5):712-717. PMID: 18585391
- Zhang Y, et al. Treatment of type 2 diabetes and dyslipidemia with the natural plant alkaloid berberine. J Clin Endocrinol Metab. 2008;93(7):2559-2565. PMID: 18397984
- Kong W, et al. Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins. Nat Med. 2004;10(12):1344-1351. PMID: 15531624
- Dong H, et al. Berberine in the treatment of type 2 diabetes mellitus: a systemic review and meta-analysis. Evid Based Complement Alternat Med. 2012;2012:591654. PMID: 22965767
- Liang Y, et al. Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: a systematic literature review and a meta-analysis. Endocr J. 2019;66(1):51-63.
- Yan HM, et al. Efficacy of berberine in patients with non-alcoholic fatty liver disease. PLoS One. 2015;10(8):e0134172. PMID: 25892123
- An Y, et al. The use of berberine for women with polycystic ovary syndrome undergoing IVF treatment. Clin Endocrinol. 2014;80(3):425-431. PMID: 24486653
- Chedid V, et al. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Glob Adv Health Med. 2014;3(3):16-24. PMID: 24891990
- Zhang X, et al. Structural changes of gut microbiota during berberine-mediated prevention of obesity and insulin resistance in high-fat diet-fed rats. PLoS One. 2012;7(8):e42529.
- Lee YS, et al. Berberine, a natural plant product, activates AMP-activated protein kinase with beneficial metabolic effects in diabetic and insulin-resistant states. Diabetes. 2006;55(8):2256-2264.
- Stermitz FR, et al. Synergy in a medicinal plant: antimicrobial action of berberine potentiated by 5'-methoxyhydnocarpin, a multidrug pump inhibitor. Proc Natl Acad Sci. 2000;97(4):1433-1437.
- Wang Y, et al. Berberine and plant stanols synergistically inhibit cholesterol absorption in hamsters. Atherosclerosis. 2010;209(2):111-117.
- Lan J, et al. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension. J Ethnopharmacol. 2015;161:69-81.
- Wei W, et al. A clinical study on the short-term effect of berberine in comparison to metformin on the metabolic characteristics of women with polycystic ovary syndrome. Eur J Endocrinol. 2012;166(1):99-105.
- Imenshahidi M, Hosseinzadeh H. Berberine and barberry (Berberis vulgaris): a clinical review. Phytother Res. 2019;33(3):504-523.
- Neag MA, et al. Berberine: botanical occurrence, traditional uses, extraction methods, and relevance in cardiovascular, metabolic, hepatic, and renal disorders. Front Pharmacol. 2018;9:557.
- Feng X, et al. Berberine in cardiovascular and metabolic diseases: from mechanisms to therapeutics. Theranostics. 2019;9(7):1923-1951.
- Kumar A, et al. Current knowledge and pharmacological profile of berberine: an update. Eur J Pharmacol. 2015;761:288-297.
- Cicero AFG, Baggioni A. Berberine and its role in chronic disease. Adv Exp Med Biol. 2016;928:27-45.
- Habtemariam S. Berberine pharmacology and the gut microbiota: a hidden therapeutic link. Pharmacol Res. 2020;155:104722.
- Boericke W. Pocket Manual of Homoeopathic Materia Medica & Repertory. 9th ed. B. Jain Publishers; 2002.
- Clarke JH. A Dictionary of Practical Materia Medica. B. Jain Publishers; 1902 (reprinted).
- Spinozzi S, et al. Berberine and its pharmacokinetic challenges: a patent review. Expert Opin Ther Pat. 2014;24(6):637-647.
- Turner N, et al. Berberine and its more biologically available derivative, dihydroberberine, inhibit mitochondrial respiratory complex I. Diabetes. 2008;57(5):1414-1418.
- Song D, et al. Biological roles of berberine: focus on its anti-inflammatory and anti-tumor mechanism. J Cell Biochem. 2020;121(2):1143-1151.
This article is for research and educational purposes. It does not constitute medical advice. Berberine is contraindicated in pregnancy, lactation, and neonates. It interacts with multiple prescription medications including metformin, statins, cyclosporine, and blood thinners. Always consult qualified healthcare providers before starting berberine supplementation, especially if you take prescription medications or have a chronic health condition.